

Epidemiology and antifungal susceptibility of bloodstream Candida isolates in Quebec: Report on 453 cases between 2003 and 2005
- PMID: 19145263
- PMCID: PMC2610277
- DOI: 10.1155/2008/634046
Epidemiology and antifungal susceptibility of bloodstream Candida isolates in Quebec: Report on 453 cases between 2003 and 2005
Abstract
Background: Between May 2003 and April 2005, a population-based surveillance of Candida bloodstream infections was conducted in Quebec. A total of 453 episodes of candidemia (464 yeast isolates) from 54 participating hospitals were studied.
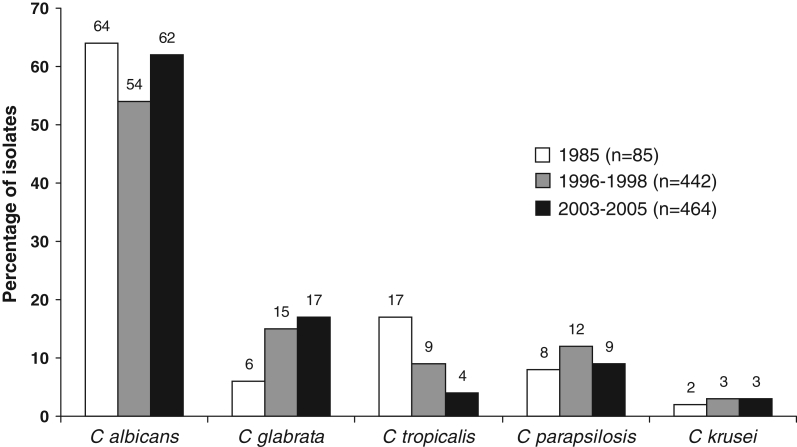
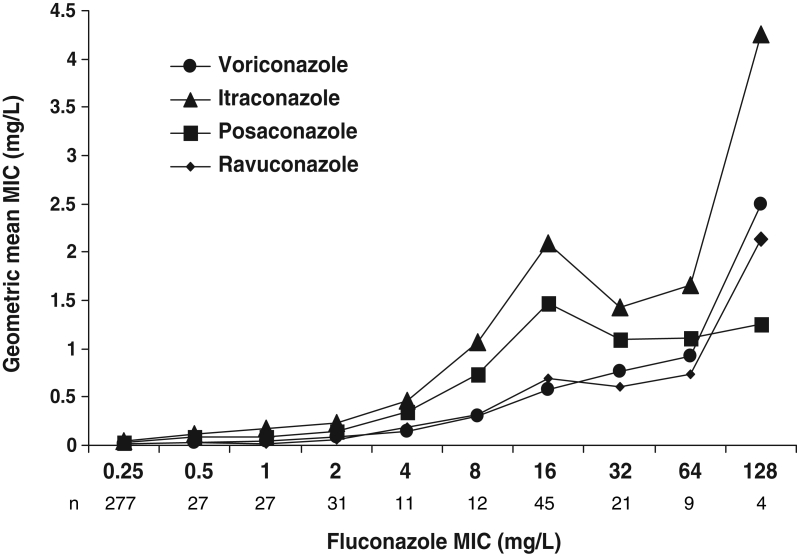
Results: The annual incidence rate was three per 100,000 population. Global hospital mortality was 38%. The most common predisposing factors were the presence of an intravascular catheter (80%), use of antibacterial therapy (67%), stay in an intensive care unit (49%), use of parenteral nutrition (32%) and intra-abdominal surgery (31%). Fluconazole alone or in association with other antifungals was used for treatment in over 80% of cases. Candida albicans comprised 62% of isolates, followed by Candida glabrata (17%), Candida parapsilosis (9%), Candida tropicalis (5%), Candida lusitaniae (3%) and Candida krusei (3%). Of the 288 C albicans isolates, seven (2%) were resistant to flucytosine, one to fluconazole and none to itraconazole or voriconazole. Of the 75 non-C albicans species isolates with reduced susceptibility to fluconazole (minimum inhibitory concentration [MIC] 16 mug/mL or greater), none were susceptible to itraconazole (MIC 0.12 mg/L or lower), whereas 71 (95%) were susceptible to voriconazole (MIC 1 mug/mL or lower). However, only five of 12 (42%) fluconazole-resistant isolates were susceptible to voriconazole. Posaconazole, ravuconazole and caspofungin displayed a broad spectrum of activity against these isolates, with MICs of 1 mg/L or lower in 56%, 92% and 100% of isolates, respectively. Overall, a correlation (r(2)>0.87) was observed among increasing fluconazole MICs and the geometric mean MICs of itraconazole, voriconazole, posaconazole and ravuconazole.
Conclusions: These surveillance results when compared with those of the 1993 to 1995 survey confirm little variation in the distribution of species causing invasive Candida infection over a 10-year period in Quebec, as well as the continuous excellent overall in vitro activity of fluconazole.
HISTORIQUE: Entre mai 2003 et avril 2005, une surveillance des cas de candidémie dans la population a été réalisée au Québec. En tout, 453 épisodes de candidémie (464 isolats de levures) provenant de 54 hôpitaux participants ont été analysés.
RÉSULTATS: L’incidence annuelle a été évaluée à trois (3) cas par 100 000 de population. La mortalité hospitalière globale a été de 38 %. Les principaux facteurs prédisposants étaient la présence d’un cathéter intravasculaire (80 %), l’utilisation d’antibactériens (67 %), un séjour en unité de soins intensifs (49 %), la nutrition parentérale (32 %) et la chirurgie abdominale (31 %). Le fluconazole, en monothérapie ou associé à d’autres antifongiques, a été utilisé pour le traitement de plus de 80 % des cas. Candida albicans représentait 62 % des isolats, suivi de Candida glabrata (17%), Candida parapsilosis (9 %), Candida tropicalis (5 %), Candida lusitaniæ (3 %) et Candida krusei (3 %). Parmi les 288 isolats de C. albicans, sept (2 %) se sont révélés résistants à la flucytosine, un au fluconazole et aucun n’a été résistant à l’itraconazole ou au voriconazole. Parmi les 75 isolats non albicans moins sensibles au fluconazole (concentrations minimales inhibitrices [CMI] 16 μg/mL ou plus), aucun n’a été sensible à l’itraconazole (CMI 0,12 mg/L ou moins), tandis que 71 (95 %) ont été sensibles au voriconazole (CMI 1 μg/mL ou moins). Par contre, seulement cinq des isolats résistants au fluconazole sur 12 (42 %) se sont révélés sensibles au voriconazole. Le posaconazole, le ravuconazole et la capsofungine ont manifesté un large spectre d’activité contre ces isolats, avec des CMI de 1 mg/L ou moins chez 56 %, 92 % et 100 % des isolats, respectivement. Dans l’ensemble, on a pu observer une corrélation (r2 > 0,87) entre les CMI croissantes du fluconazole et les moyennes géométriques des CMI de l’itraconazole, du voriconazole, du posaconazole et du ravuconazole.
CONCLUSIONS: Comparativement aux résultats de la surveillance exercée entre 1993 à 1995, cette analyse confirme que la distribution des espèces de Candida responsables d’infections invasives a peu varié au Québec en dix ans et que le fluconazole conserve une excellente activité globale in vitro.
Keywords: Antifungal resistance; Candidemia; Surveillance.
Figures
References
-
- Beck-Sagué C, Jarvis WR. Secular trends in the epidemiology of nosocomial fungal infections in the United States, 1980–1990. National Nosocomial Infections Surveillance System. J Infect Dis. 1993;167:1247–51. - PubMed
-
- Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. Nosocomial bloodstream infections in United States hospitals: A three-year analysis. Clin Infect Dis. 1999;29:239–44. - PubMed
-
- Golan Y, Wolf MP, Pauker SG, Wong JB, Hadley S. Empirical anti-Candida therapy among selected patients in the intensive care unit: A cost-effectiveness analysis. Ann Intern Med. 2005;143:857–69. - PubMed
-
- Morgan J, Meltzer MI, Plikaytis BD, et al. Excess mortality, hospital stay, and cost due to candidemia: A case-control study using data from population-based candidemia surveillance. Infect Control Hosp Epidemiol. 2005;26:540–7. (Erratum in 2005;26:675) - PubMed
-
- Zaoutis TE, Argon J, Chu J, Berlin JA, Walsh TJ, Feudtner C. The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: A propensity analysis. Clin Infect Dis. 2005;41:1232–9. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
