

Review
doi: 10.1016/j.bbmt.2008.10.027.
Plasma biomarkers in graft-versus-host disease: a new era?
Affiliations
- PMID: 19147075
- PMCID: PMC2644447
- DOI: 10.1016/j.bbmt.2008.10.027
Item in Clipboard
Review
Plasma biomarkers in graft-versus-host disease: a new era?
Biol Blood Marrow Transplant.
2009 Jan.
Abstract
Acute graft versus host disease (GVHD) remains a major complication of allogeneic hematopoietic cell transplantation (HCT). The diagnosis of acute GVHD is based on strictly clinical criteria and its severity also determined by these criteria. Currently, there is no validated diagnostic blood test for acute GVHD. This review will summarize proteomics approaches to identify biomarkers for GVHD in the plasma with diagnostic, prognostic and predictive value. If successful, these studies could establish a novel biomarker panel that will contribute important information including long term survival, and that may eventually facilitate therapeutic decisions for allogeneic HCT patients.
Figures
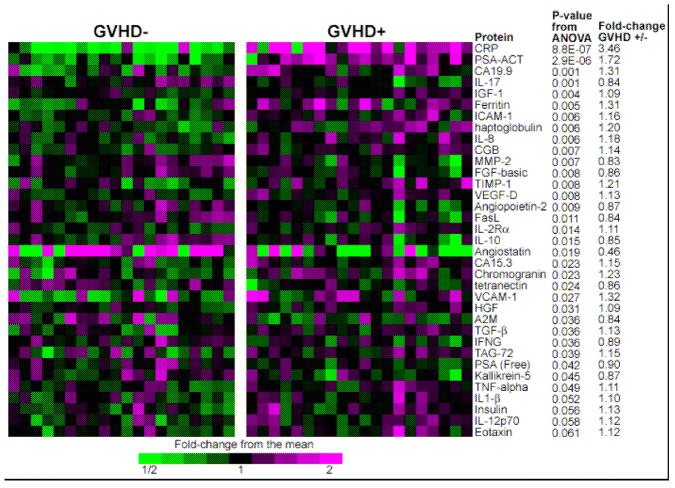
This heatmap depicts relative protein values obtained from antibody microarrays after removal of batch effects due to three separate analyses. Samples from 21 GVHD–patients (left panel) and 21 GVHD+ patients (right panel) are represented. Only the antibodies giving the 35 smallest p-values for differences between GVHD+ and GVHD– patient plasma are shown. P-values compare GVHD+ and GVHD–samples. Reproduced with permission from reference .
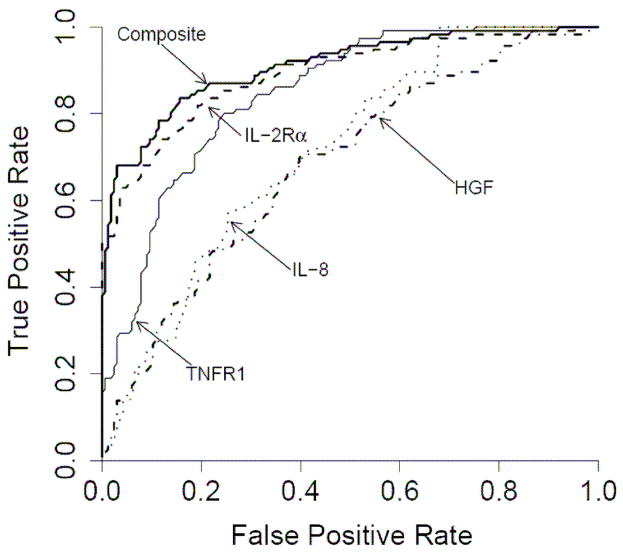
Individual ROC curves for IL-2Rα (- - - -), TNFR1 (——), HGF ( ) and IL-8 (
) and IL-8 ( ) and the composite panel (———). Reproduced with permission from reference .
) and the composite panel (———). Reproduced with permission from reference .
) and IL-8 () and the composite panel (———). Reproduced with permission from reference .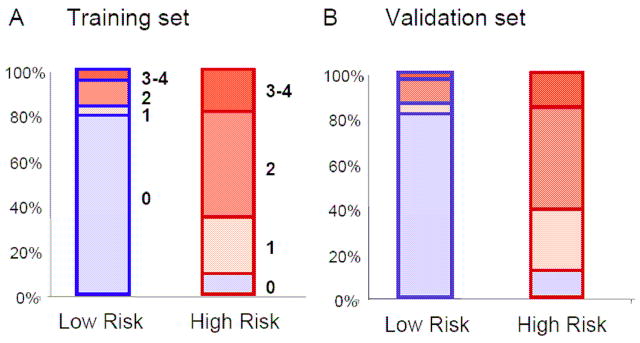
The blue boxes represent the low risk groups and the red boxes the high risk groups in the training (Panel A) and validation (Panel B) sets. The filled blue colors represent the GVHD grade 0 and the filled red colors the GVHD grade 1–4.
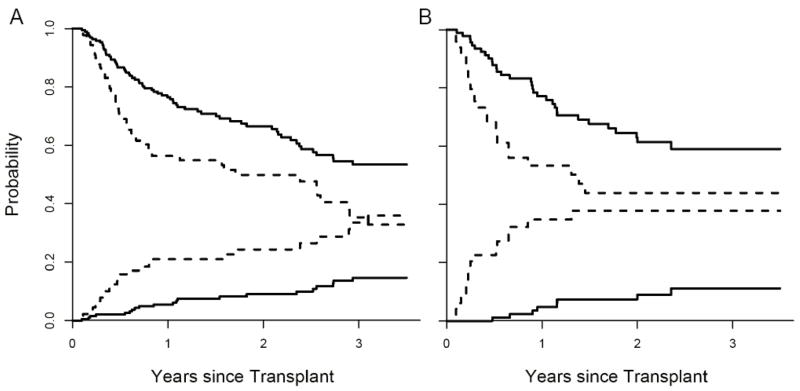
In Panel A, the cumulative incidence of NRM and OS (determined by Kaplan Meier) are plotted according to the predicted probability of acute GVHD: low (—, n = 193) and high (- - -, n = 89). P = 0.001 and 0.006 (adjusted for age, donor type, HLA-match and intensity of conditioning) for differences in NRM and OS, respectively. The NRM at 3.5 years is 15% [95% CI, 9%–21%] for the low risk group and 36% [95% CI, 24%–48%] for the high risk group. OS at 3.5 years is 53% [95% CI, 45%–63%] for the low risk group and 33% [95% CI, 22%–48%] in the high risk group. In Panel B, the cumulative incidence of NRM and OS of the two groups are plotted for the validation set: low (—, n = 93) and high (- - -, n = 49). P < 0.001 and 0.02 (adjusted as before) for differences in NRM and OS, respectively. The NRM at 3.5 years is 11% [95% CI, 4%–19%] for the low risk group and 38% [95% CI, 23%–53%] for the high risk group. OS at 3.5 years is 59% [95% CI, 49%–72%] for the low risk group and 44%, [95% CI, 31%–63%] for the high risk group. Reproduced with permission from reference .
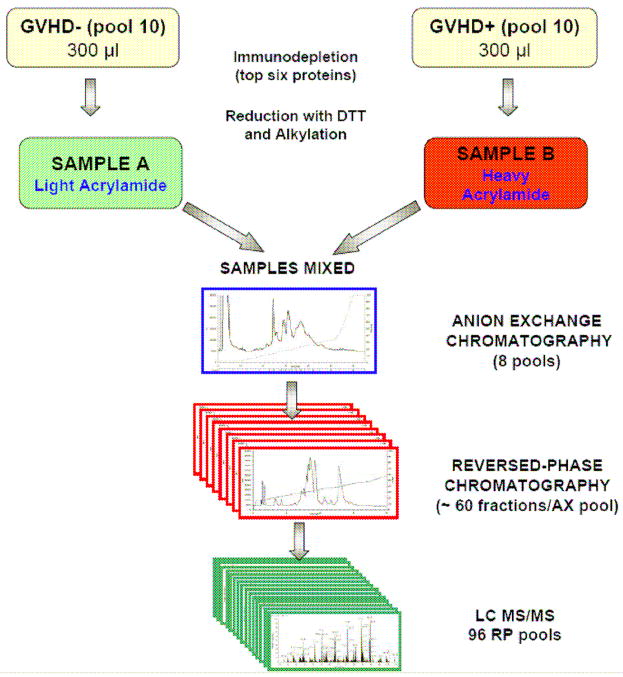
Plasma pooled from ten patients with GVHD are labeled with the heavy isotope and compared to plasma pooled from ten patients with no GVHD labeled with the light isotope. The specimens are then subjected to extensive fractionation (by ion-exchange chromatography and reversed-phase chromatography) before analysis of individual fractions. The result is a reduced complexity of individual fractions subjected to analysis by liquid chromatography – tandem mass spectrometry (LC-MS/MS). Adapted from reference .
References
-
- Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15:825–828. - PubMed
-
- Martin PJ, Schoch G, Fisher L, et al. A retrospective analysis of therapy for acute graft-versus-host disease: secondary treatment. Blood. 1991;77:1821–1828. - PubMed
-
- Miyamoto T, Akashi K, Hayashi S, et al. Serum concentration of the soluble interleukin-2 receptor for monitoring acute graft-versus-host disease. Bone Marrow Transplant. 1996;17:185–190. - PubMed
-
- Grimm J, Zeller W, Zander AR. Soluble interleukin-2 receptor serum levels after allogeneic bone marrow transplantations as a marker for GVHD. Bone Marrow Transplant. 1998;21:29–32. - PubMed
-
- Foley R, Couban S, Walker I, et al. Monitoring soluble interleukin-2 receptor levels in related and unrelated donor allogenic bone marrow transplantation. Bone Marrow Transplant. 1998;21:769–773. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
