

Enhanced myogenic constriction of mesenteric artery in heart failure relates to decreased smooth muscle cell caveolae numbers and altered AT1- and epidermal growth factor-receptor function
- PMID: 19147448
- PMCID: PMC2645056
- DOI: 10.1093/eurjhf/hfn027
Enhanced myogenic constriction of mesenteric artery in heart failure relates to decreased smooth muscle cell caveolae numbers and altered AT1- and epidermal growth factor-receptor function
Abstract
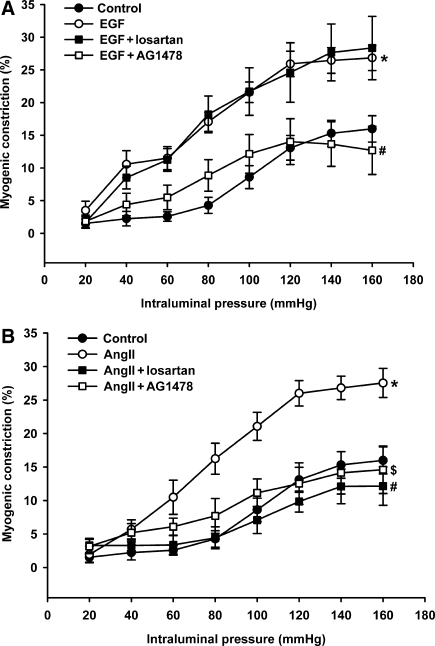
Aims: We previously showed that enhanced myogenic constriction (MC) of peripheral resistance arteries involves active AT(1) receptors in chronic heart failure (CHF). Recent data suggest both transactivation of EGF receptors and caveolae-like microdomains to be implicated in the activity of AT(1) receptors. Thus, we assessed their roles in increased MC in mesenteric arteries of CHF rats.
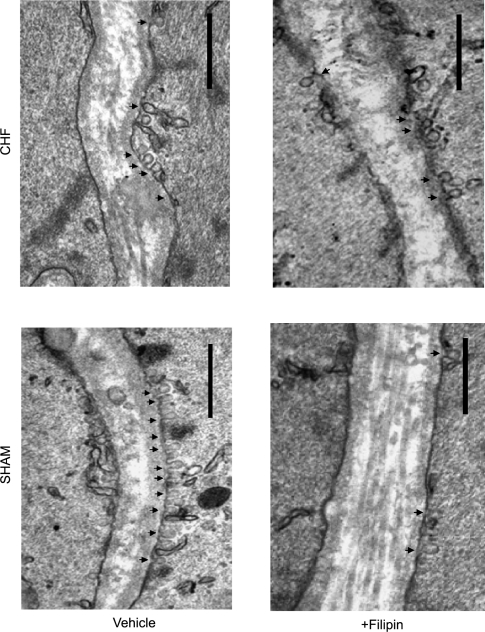
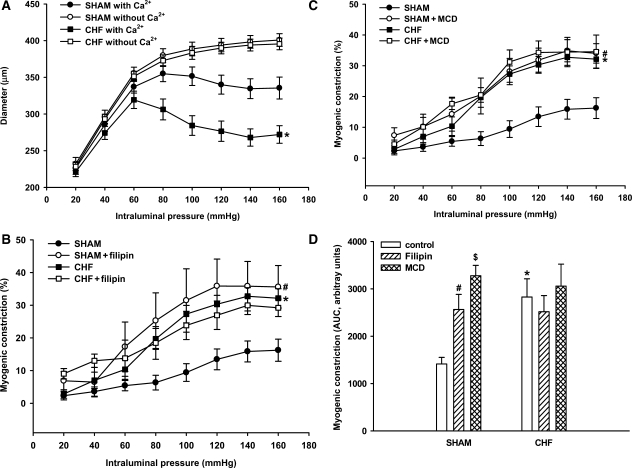
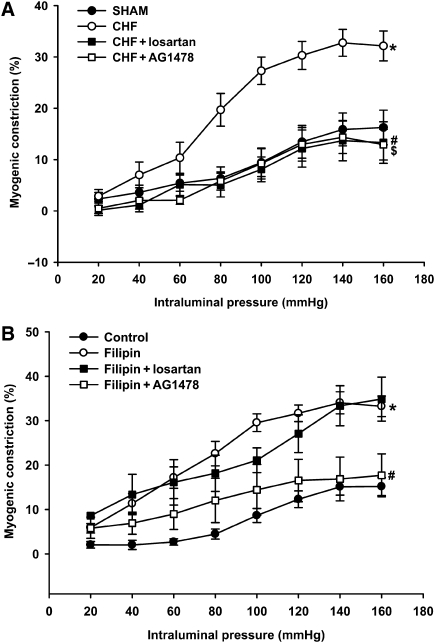
Methods and results: Male Wistar rats underwent myocardial infarction to induce CHF and were sacrificed after 12 weeks. The number of caveolae in smooth muscle cells (SMC) of mesenteric arteries of CHF rats was decreased by 43.6 +/- 4.0%, this was accompanied by increased MC, which was fully normalized to the level of sham by antagonists of the AT(1)-receptor (losartan) or EGF-receptor (AG1478). Acute disruption of caveolae in sham rats affected caveolae numbers and MC to a similar extent as CHF, however MC was only reversed by the antagonist of the EGF-receptor, but not by the AT(1)-receptor antagonist. Further, in sham rats, MC was increased by a sub-threshold concentration of angiotensin II and reversed by both AT(1)- as well as EGF-receptor inhibition. In contrast, increased MC by a sub-threshold concentration of EGF was only reversed by EGF receptor inhibition.
Conclusion: These findings provide the first evidence that decreased SMC caveolae numbers are involved in enhanced MC in small mesenteric arteries, by affecting AT(1)- and EGF-receptor function. This suggests a novel mechanism involved in increased peripheral resistance in CHF.
Figures
References
-
- Schrier RW, Abraham WT. Mechanisms of disease - Hormones and hemodynamics in heart failure. N Eng J Med. 1999;341:577–585. - PubMed
-
- Davis MJ, Hill MA. Signaling mechanisms underlying the vascular myogenic response. Physiol Rev. 1999;79:387–423. - PubMed
-
- Kagiyama S, Eguchi S, Frank GD, Inagami T, Zhang YC, Phillips MI. Angiotensin II-induced cardiac hypertrophy and hypertension are attenuated by epidermal growth factor receptor antisense. Circulation. 2002;106:909–912. - PubMed
-
- Ushio-Fukai M, Hilenski L, Santanam N, Becker PL, Ma Y, Griendling KK, Alexander RW. Cholesterol depletion inhibits epidermal growth factor receptor transactivation by angiotensin II in vascular smooth muscle cells: role of cholesterol-rich microdomains and focal adhesions in angiotensin II signaling. J Biol Chem. 2001;276:48269–48275. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
