

Assessment of safety and long-term outcomes of initial treatment with placebo in TADS
- PMID: 19147693
- PMCID: PMC2823118
- DOI: 10.1176/appi.ajp.2008.08040487
Assessment of safety and long-term outcomes of initial treatment with placebo in TADS
Abstract
Objective: The authors examined whether initial assignment to receive placebo for 12 weeks followed by open active treatment as clinically indicated was associated with different levels of benefit and risk of harm across 36 weeks as compared with initial assignment to receive active treatments.
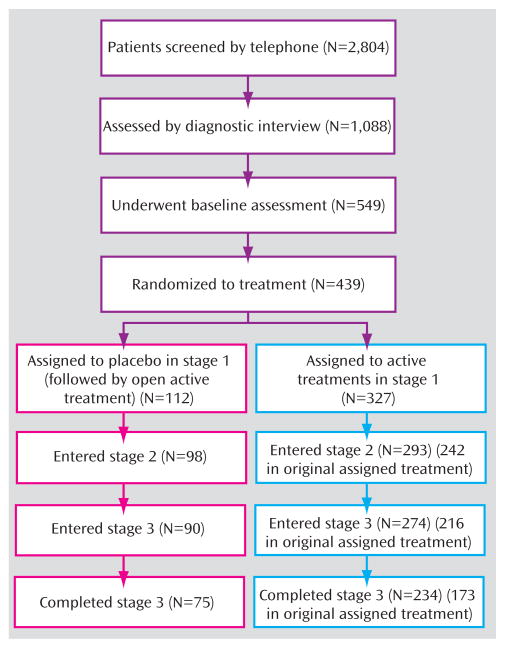
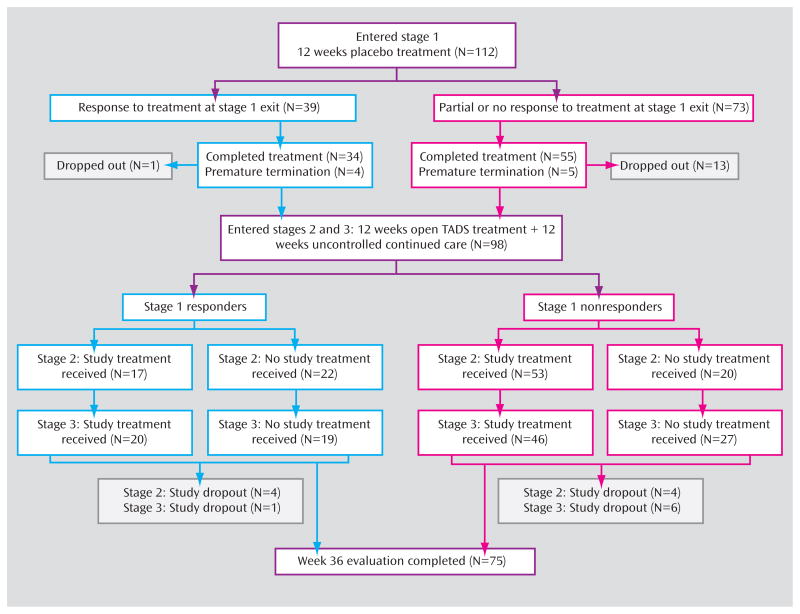
Method: Adolescents with major depressive disorder (N=439) were randomly assigned to receive an initial 12 weeks of treatment with fluoxetine, cognitive-behavioral therapy (CBT), combination treatment with fluoxetine and CBT, or clinical management with placebo; those assigned to placebo received open active treatment as clinically indicated after 12 weeks of placebo. Assessments were conducted every 6 weeks for 36 weeks. The primary outcome measures were response and remission based on scores on the Children's Depression Rating Scale-Revised and the Clinical Global Impression improvement subscale.
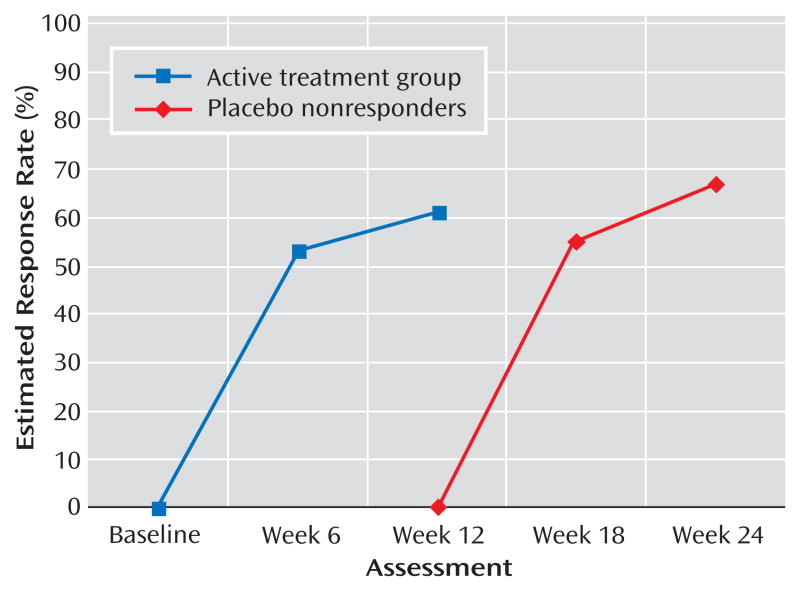
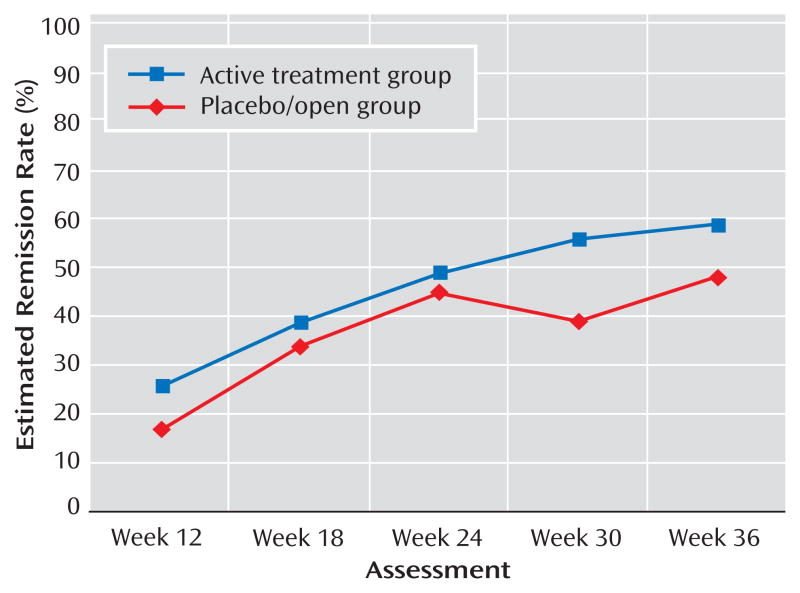
Results: At week 36, the response rate was 82% in the placebo/open group and 83% in the active treatment groups. The remission rate was 48% in the placebo/open group and 59% in the active treatment groups, a difference that approached statistical significance. Patients who responded to placebo generally retained their response. Those who did not respond to placebo subsequently responded to active treatment at the same rate as those initially assigned to active treatments. There were no differences between groups in rates of suicidal events, study retention, or symptom worsening.
Conclusions: Remission rates at 9 months were lower in patients treated initially with placebo, but 3 months of placebo treatment was not associated with any harm or diminished response to subsequent treatment.
Figures
References
-
- Charney DS, Nemeroff CB, Lewis L, Laden SK, Gorman JM, Laska EM, Borenstein M, Bowden CL, Caplan A, Emslie GJ, Evans DL, Geller B, Grabowski LE, Herson J, Kalin NH, Keck PE, Jr, Kirsch I, Krishnan KR, Kupfer DJ, Makuch RW, Miller FG, Pardes H, Post R, Reynolds MM, Roberts L, Rosenbaum JF, Rosenstein DL, Rubinow DR, Rush AJ, Ryan ND, Sachs GS, Schatzberg AF, Solomon S Consensus Development Panel. National Depressive and Manic-Depressive Association consensus statement on the use of placebo in clinical trials of mood disorders. Arch Gen Psychiatry. 2002;59:262–270. - PubMed
-
- Khan A, Warner HA, Brown WA. Symptom reduction and suicide risk in patients treated with placebo in antidepressant clinical trials: an analysis of the Food and Drug Administration database. Arch Gen Psychiatry. 2000;57:311–317. - PubMed
-
- Emslie GJ, Ryan ND, Wagner KD. Major depressive disorder in children and adolescents: clinical trial design and antidepressant efficacy. J Clin Psychiatry. 2005;66:14–20. - PubMed
-
- Derivan AT, Leventhal BL, March J, Wolraich M, Zito JM. The ethical use of placebo in clinical trials involving children. J Child Adolesc Psychopharmacol. 2004;14:167–174. - PubMed
-
- March J, Kratochvil C, Clarke G, Beardslee W, Derivan A, Emslie G, Green EP, Heiligenstein J, Hinshaw S, Hoagwood K, Jensen P, Lavori P, Leonard H, McNulty J, Michaels MA, Mossholder A, Osher T, Petti T, Prentice E, Vitiello B, Wells K. AACAP 2002 research forum: placebo and alternatives to placebo in randomized controlled trials in pediatric psychopharmacology. J Am Acad Child Adolesc Psychiatry. 2004;43:1046–1056. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
