

Graves ophthalmopathy: the bony orbit in optic neuropathy, its apical angular capacity, and impact on prediction of risk
- PMID: 19147718
- PMCID: PMC7051464
- DOI: 10.3174/ajnr.A1413
Graves ophthalmopathy: the bony orbit in optic neuropathy, its apical angular capacity, and impact on prediction of risk
Abstract
Background and purpose: Optic neuropathy (ON), a serious complication of Graves ophthalmopathy, is often subclinical and masked by symptoms of orbitopathy. We examined herein bony and soft-tissue CT features associated with ON, including an angular assessment of orbital apex capacity, and their usefulness in the risk prediction of ON.
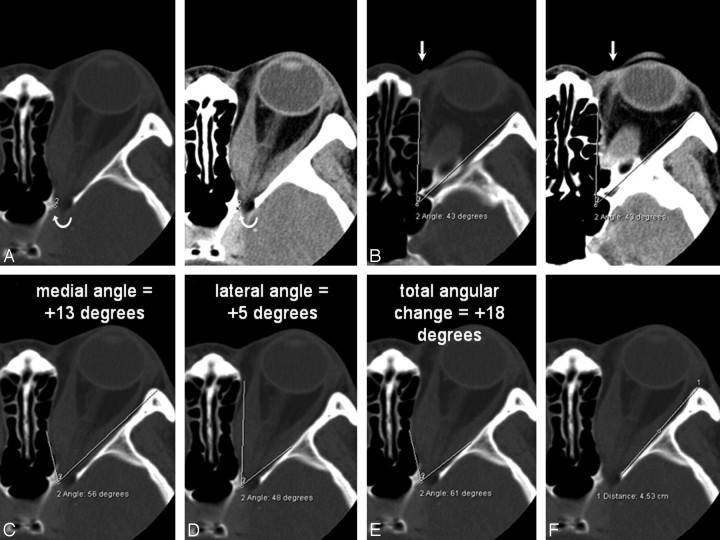
Materials and methods: The CT scans of 41 patients with Graves ophthalmopathy (17 men, 24 women; mean age, 49.1 years) clinically diagnosed with (19 patients, 32 orbits) or without ON were evaluated by 2 independent raters. Quantitative linear and angular measurements of the orbital structures and bony walls and categoric scores of apical crowding and intracranial fat prolapse were assessed on a clinical workstation. Inter- and intrarater variability of these features was determined. The CT features of the 2 patient groups were compared, and multivariate logistic regression analysis was performed to evaluate the predictive features of ON.
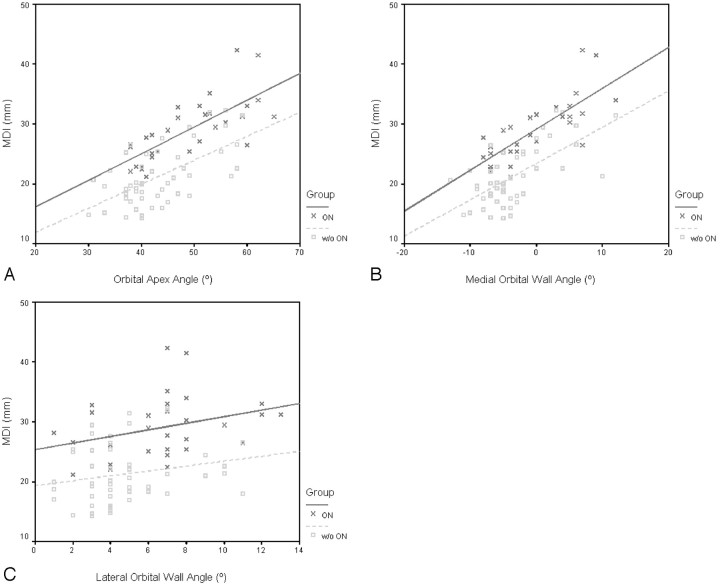
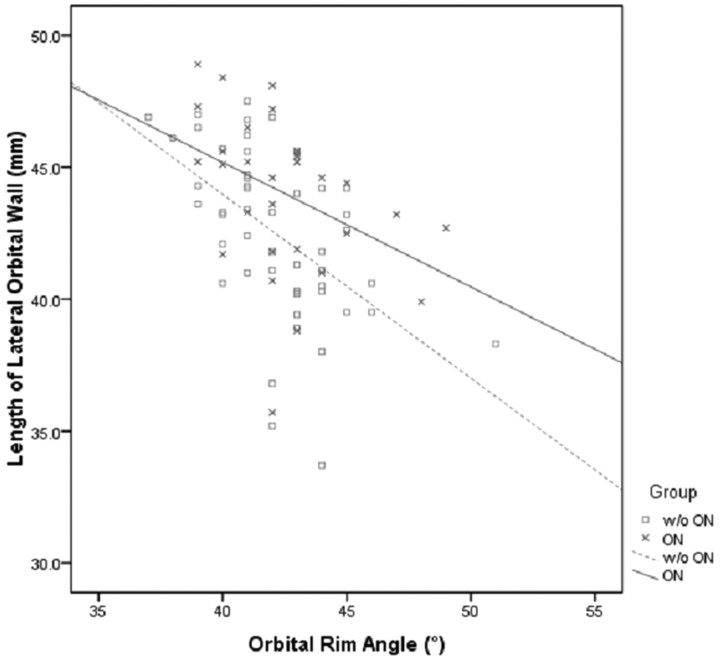
Results: Bony orbital angles (P < .005), length of the lateral orbital wall (P < .05), muscular diameters (P < .0005), muscular bulk of the medial rectus muscle relative to the bony orbit (P < .05), and apical crowding (P < .0005) were associated with clinical ON. Stepwise multivariate logistic regression analysis revealed the muscle diameter index and medial and lateral wall angles to be independent predictors. Combining these in a single multivariate equation yielded sensitivity, specificity, and positive and negative predictive values of 73%, 90%, 82%, and 85%, respectively.
Conclusions: Orbital wall angles, especially the medial wall, and muscular enlargement are independent risk predictors.
Figures

Similar articles
-
Quantitative computed tomographic predictors of compressive optic neuropathy in patients with thyroid orbitopathy: a volumetric analysis.Ophthalmology. 2012 Oct;119(10):2174-8. doi: 10.1016/j.ophtha.2012.04.021. Epub 2012 Jun 17. Ophthalmology. 2012. PMID: 22709420
-
Risk prediction of dysthyroid optic neuropathy based on CT imaging features combined the bony orbit with the soft tissue structures.Front Med (Lausanne). 2022 Aug 24;9:936819. doi: 10.3389/fmed.2022.936819. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36091692 Free PMC article.
-
Predicting dysthyroid optic neuropathy using computed tomography volumetric analyses of orbital structures.Clinics (Sao Paulo). 2012 Aug;67(8):891-6. doi: 10.6061/clinics/2012(08)06. Clinics (Sao Paulo). 2012. PMID: 22948455 Free PMC article.
-
Optic neuropathy following orbital irradiation for Graves' ophthalmopathy: a case report and literature review.Orbit. 2012 Feb;31(1):30-3. doi: 10.3109/01676830.2011.603458. Epub 2011 Oct 26. Orbit. 2012. PMID: 22029640 Review.
-
Neuroimaging of Graves' orbitopathy.Best Pract Res Clin Endocrinol Metab. 2012 Jun;26(3):259-71. doi: 10.1016/j.beem.2011.11.009. Best Pract Res Clin Endocrinol Metab. 2012. PMID: 22632363 Review.
Cited by
-
Imaging studies for diagnosing Graves' orbitopathy and dysthyroid optic neuropathy.Clinics (Sao Paulo). 2012 Nov;67(11):1327-34. doi: 10.6061/clinics/2012(11)18. Clinics (Sao Paulo). 2012. PMID: 23184212 Free PMC article. Review.
-
The diagnostic value of the IDEAL-T2WI sequence in dysthyroid optic neuropathy: a quantitative analysis of the optic nerve and cerebrospinal fluid in the optic nerve sheath.Eur Radiol. 2021 Oct;31(10):7419-7428. doi: 10.1007/s00330-021-08030-5. Epub 2021 May 15. Eur Radiol. 2021. PMID: 33993334
-
Assessment of Orbital Computed Tomography (CT) Imaging Biomarkers in Patients with Thyroid Eye Disease.J Digit Imaging. 2019 Dec;32(6):987-994. doi: 10.1007/s10278-019-00195-2. J Digit Imaging. 2019. PMID: 31197558 Free PMC article.
-
Predictive parameters on CT scan for dysthyroid optic neuropathy.Int J Ophthalmol. 2020 Aug 18;13(8):1266-1271. doi: 10.18240/ijo.2020.08.13. eCollection 2020. Int J Ophthalmol. 2020. PMID: 32821681 Free PMC article.
-
Graves' ophthalmopathy.N Engl J Med. 2010 Feb 25;362(8):726-38. doi: 10.1056/NEJMra0905750. N Engl J Med. 2010. PMID: 20181974 Free PMC article. Review.
References
-
- Rootman J, Dolman P. Thyroid orbitopathy. In: Rootman J, ed. Diseases of the Orbit: A Multidiciplinary Approach. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;2003. :182–86
-
- Trobe JD. Optic nerve involvement in dysthyroidism. Ophthalmology 1981;88:488–92 - PubMed
-
- Barrett L, Glatt HJ, Burde RM, et al. Optic nerve dysfunction in thyroid eye disease: CT. Radiology 1988;167:503–07 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous