

Practice Guideline
doi: 10.1016/s0828-282x(09)70019-4.
Canadian Cardiovascular Society Working Group: Providing a perspective on the 2007 focused update of the American College of Cardiology and American Heart Association 2004 guidelines for the management of ST elevation myocardial infarction
Affiliations
- PMID: 19148339
- PMCID: PMC2691877
- DOI: 10.1016/s0828-282x(09)70019-4
Item in Clipboard
Practice Guideline
Canadian Cardiovascular Society Working Group: Providing a perspective on the 2007 focused update of the American College of Cardiology and American Heart Association 2004 guidelines for the management of ST elevation myocardial infarction
Can J Cardiol.
2009 Jan.
No abstract available
Figures
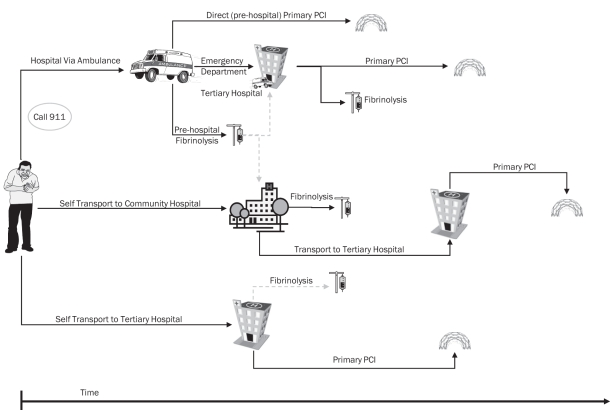
Assessing time to treatment from point of first medical contact. This figure schematically presents reperfusion options and their associated time to treatment measured from first medical contact. In patients who activate the prehospital emergency medical system, treatment delays can be reduced through the use of prehospital fibrinolysis or direct triage to a cardiac catheterization tertiary care centre that is capable of delivering timely primary percutaneous coronary intervention (PCI). In patients who self-transport to a tertiary care hospital emergency department, rapid delivery of primary PCI is the treatment of choice, with fibrinolysis maintained as an alternative. In patients who self-transport to a community hospital, transfer for primary PCI has been employed, although fibrinolysis may be considered reasonable because challenges remain in achieving timely primary PCI. In all situations, first medical contact (either arrival of the ambulance at the scene or patient arrival at the hospital) is the point from which the treatment is tracked
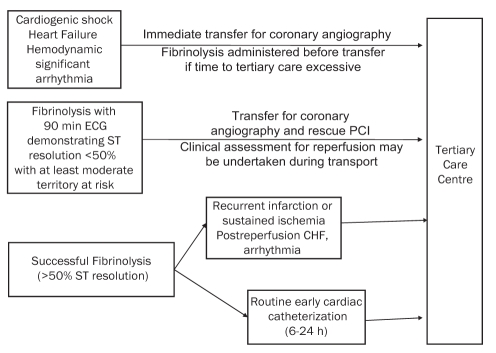
Community ST elevation myocardial infarction patients requiring transfer to a tertiary care centre. Suggestions regarding appropriate transfer of patients to a tertiary care centre (region) following presentation to a community hospital (where primary percutaneous coronary intervention [PCI] cannot be achieved) are presented. In patients who present with (or develop) cardiogenic shock, heart failure or hemodynamically significant arrhythmia, immediate transfer to a centre capable of acute revascularization should occur. Patients should be transferred to a tertiary care centre after receiving fibrinolysis if they fail to achieve adequate reperfusion, as defined by a less than 50% ST segment resolution on a 90 min electrocardiogram (ECG) in association with at least a moderate territory of myocardium at risk. In patients who achieve successful reperfusion following fibrinolysis, preliminary evidence suggests there is benefit from routine cardiac catheterization and revascularization completed within 6 h to 24 h. In patients who develop recurrent infarction, sustained ischemia or high-risk features during convalescence, transfer to a tertiary care centre for cardiac catheterization and revascularization is appropriate. CHF Congestive heart failure
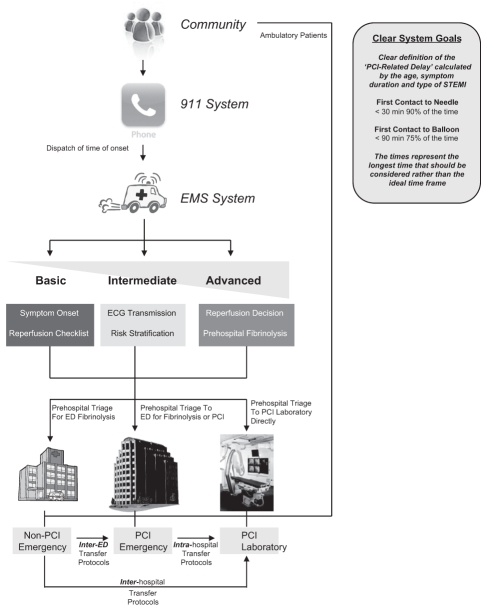
Systems approach to ST elevation myocardial infarction (STEMI). ECG Electrocardiogram; ED Emergency department; EMS Emergency medical services; PCI Percutaneous coronary intervention
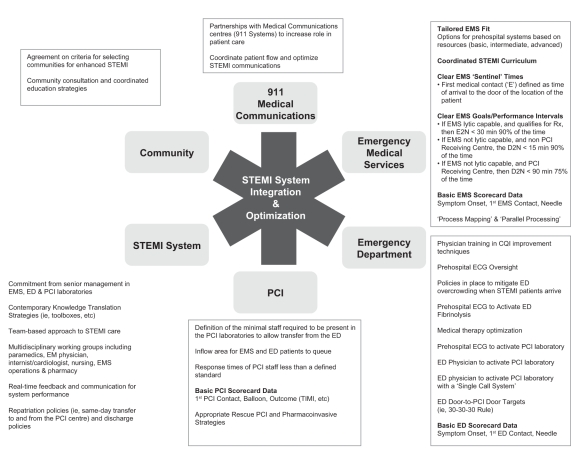
System requirements for ST elevation myocardial infarction (STEMI) care in Canada. CQI Continuous quality improvement; D2N Emergency door to needle (administration of fibrinolysis); E2N EMS arrival (first medical contact) to needle (administration of fibrinolysis); ECG Electrocardiogram; ED Emergency department; EM Emergency medicine; EMS Emergency medical services; PCI Percutaneous coronary intervention; Rx Prescription; TIMI Thrombolysis In Myocardial Infarction
References
-
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction) J Am Coll Cardiol. 2004;44:E1–211. - PubMed
-
- Armstrong PW, Bogaty P, Buller CE, Dorian P, O’Neill BJ. The 2004 ACC/AHA Guidelines: A perspective and adaptation for Canada by the Canadian Cardiovascular Society Working Group. Can J Cardiol. 2004;20:1075–9. - PubMed
-
- Antman EM, Hand M, Armstrong PW, et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2008;117:296–329. - PubMed
-
- Chen ZM, Pan HC, Chen YP, et al. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: Randomised placebo-controlled trial. Lancet. 2005;366:1622–32. - PubMed
-
- Boden WE, Eagle K, Granger CB. Reperfusion strategies in acute ST-segment elevation myocardial infarction: A comprehensive review of contemporary management options. J Am Coll Cardiol. 2007;50:917–29. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
