

Radical cyberknife radiosurgery with tumor tracking: an effective treatment for inoperable small peripheral stage I non-small cell lung cancer
- PMID: 19149899
- PMCID: PMC2647945
- DOI: 10.1186/1756-8722-2-1
Radical cyberknife radiosurgery with tumor tracking: an effective treatment for inoperable small peripheral stage I non-small cell lung cancer
Abstract
Objective: Curative surgery is not an option for many patients with clinical stage I non-small-cell lung carcinoma (NSCLC), but radical radiosurgery may be effective.
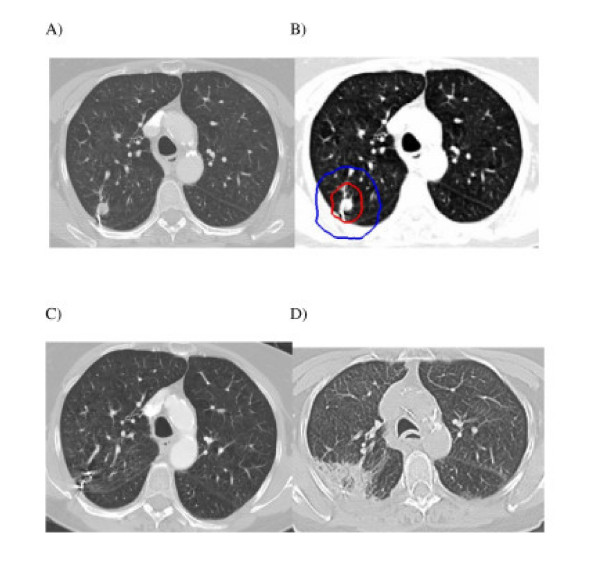
Methods: Inoperable patients with small peripheral clinical stage I NSCLC were enrolled in this study. Three-to-five fiducial markers were implanted in or near tumors under CT guidance. Gross tumor volumes (GTVs) were contoured using lung windows. The GTV margin was expanded by 5 mm to establish the planning treatment volume (PTV). A dose of 42-60 Gy was delivered to the PTV in 3 equal fractions in less than 2 weeks using the CyberKnife radiosurgery system. The 30-Gy isodose contour extended at least 1 cm from the GTV. Physical examination, CT imaging and pulmonary function testing were completed at 6 months intervals for three years following treatment.
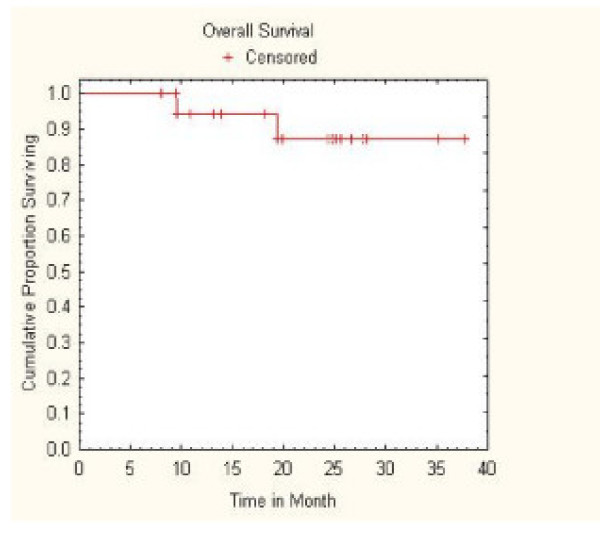
Results: Twenty patients with an average maximum tumor diameter of 2.2 cm (range, 1.1 - 3.5 cm) and a mean FEV1 of 1.08 liters (range, 0.53 - 1.71 L) were treated. Pneumothorax requiring tube thoracostomy occurred following CT-guided fiducial placement in 25% of the patients. All patients completed treatment with few acute side effects and no procedure-related mortality. Transient chest wall discomfort developed in 8 of the 12 patients with lesions within 5 mm of the pleura. The mean percentage of the total lung volume receiving a minimum of 15 Gy was 7.3% (range, 2.4% to 11.3%). One patient who received concurrent gefitinib developed short-lived, grade III radiation pneumonitis. The mean percent predicted DLCO decreased by 9% and 11% at 6 and 12 months, respectively. There were no local failures, regional lymph node recurrences or distant metastases. With a median follow-up of 25 months for the surviving patients, Kaplan-Meier overall survival estimate at 2 years was 87%, with deaths due to COPD progression.
Conclusion: Radical CyberKnife radiosurgery is a well-tolerated treatment option for inoperable patients with small, peripheral stage I NSCLC. Effective doses and adequate margins are likely to have contributed to the optimal early local control seen in this study.
Figures
References
-
- Allen MS, Darling GE, Pechet TT, Mitchell JD, Herndon JE, 2nd, Landreneau RJ, Inculet RI, Jones DR, Meyers BF, Harpole DH, Putnam JB, Jr, Rusch VW. Morbidity and mortality of major pulmonary resections in patients with early-stage lung cancer: initial results of the randomized, prospective ACOSOG Z0030 trial. Ann Thorac Surg. 2006;81:1013–1019. doi: 10.1016/j.athoracsur.2005.06.066. discussion 1019–1020. - DOI - PubMed
-
- El-Sherif A, Gooding WE, Santos R, Pettiford B, Ferson PF, Fernando HC, Urda SJ, Luketich JD, Landreneau RJ. Outcomes of sublobar resection versus lobectomy for stage I non-small cell lung cancer: a 13-year analysis. Ann Thorac Surg. 2006;82:408–415. doi: 10.1016/j.athoracsur.2006.02.029. discussion 415–406. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
