

Intussusception of the bowel in adults: a review
- PMID: 19152443
- PMCID: PMC2653360
- DOI: 10.3748/wjg.15.407
Intussusception of the bowel in adults: a review
Abstract
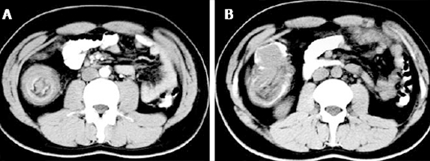
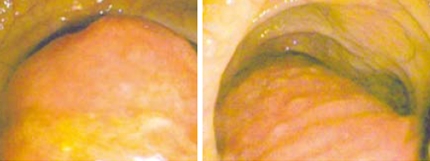
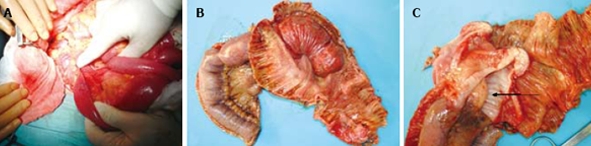
Intussusception of the bowel is defined as the telescoping of a proximal segment of the gastrointestinal tract within the lumen of the adjacent segment. This condition is frequent in children and presents with the classic triad of cramping abdominal pain, bloody diarrhea and a palpable tender mass. However, bowel intussusception in adults is considered a rare condition, accounting for 5% of all cases of intussusceptions and almost 1%-5% of bowel obstruction. Eight to twenty percent of cases are idiopathic, without a lead point lesion. Secondary intussusception is caused by organic lesions, such as inflammatory bowel disease, postoperative adhesions, Meckel's diverticulum, benign and malignant lesions, metastatic neoplasms or even iatrogenically, due to the presence of intestinal tubes, jejunostomy feeding tubes or after gastric surgery. Computed tomography is the most sensitive diagnostic modality and can distinguish between intussusceptions with and without a lead point. Surgery is the definitive treatment of adult intussusceptions. Formal bowel resection with oncological principles is followed for every case where a malignancy is suspected. Reduction of the intussuscepted bowel is considered safe for benign lesions in order to limit the extent of resection or to avoid the short bowel syndrome in certain circumstances.
Figures
References
-
- de Moulin D. Paul Barbette, M.D.: a seventeenth-century Amsterdam author of best-selling textbooks. Bull Hist Med. 1985;59:506–514. - PubMed
-
- Noble I. Master surgeon: John Hunter. J. Messner: New York; 1971. p. 185.
-
- Hutchinson H, Hutchinson J. Jonathan Hutchinson, life and letters. 1st ed. Wm Heinemann Medical Books: London; 1946.
-
- Weilbaecher D, Bolin JA, Hearn D, Ogden W 2nd. Intussu-sception in adults. Review of 160 cases. Am J Surg. 1971;121:531–535. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
