

Improved glycaemic control by switching from insulin NPH to insulin glargine: a retrospective observational study
- PMID: 19152692
- PMCID: PMC2637245
- DOI: 10.1186/1475-2840-8-3
Improved glycaemic control by switching from insulin NPH to insulin glargine: a retrospective observational study
Abstract
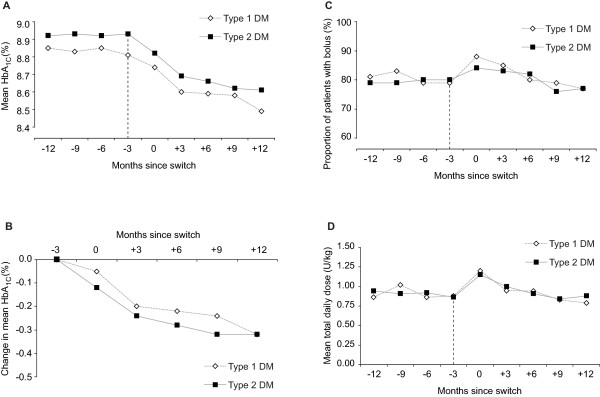
Background: Insulin glargine (glargine) and insulin NPH (NPH) are two basal insulin treatments. This study investigated the effect on glycaemic control of switching from a NPH-based regimen to a glargine-based regimen in 701 patients with type 1 (n= 304) or type 2 (n= 397) diabetes, using unselected primary care data.
Methods: Data for this retrospective observational study were extracted from a UK primary care database (The Health Improvement Network). Patients were required to have at least 12 months of data before and after switching from NPH to glargine. The principal analysis was the change in HbA(1c) after 12 months treatment with glargine; secondary analyses included change in weight and total daily insulin dose. Inconsistent reporting of hypoglycemic episodes precludes reliable reporting of this outcome. Multivariate analyses were used to adjust for baseline characteristics and confounding variables.
Results: After adjustment, both diabetic cohorts showed statistically significant reductions in mean HbA(1c) 12 months after the switch, by 0.38% (p < 0.001) in type 1 patients and 0.31% (p < 0.001) in type 2 patients. Improvement in HbA1c was positively correlated with baseline HbA(1c); patients with baseline HbA(1c) > or = 8% had reductions of 0.57% (p < 0.001) and 0.47% (p < 0.001), respectively. There was no significant change in weight or total daily insulin dose while on glargine. The majority of patients received a basal-bolus regimen prior to and after the switch (mean 79.3% before and 77.2% after switch in type 1 patients, and 80.4% and 76.8%, respectively in type 2 patients, p > 0.05).
Conclusion: In routine clinical practice, switching from NPH to glargine provides the opportunity for improving glycaemic control in diabetes patients inadequately controlled by NPH.
Figures
Similar articles
-
Switching from premixed insulin to glargine-based insulin regimen improves glycaemic control in patients with type 1 or type 2 diabetes: a retrospective primary-care-based analysis.Cardiovasc Diabetol. 2009 Feb 16;8:9. doi: 10.1186/1475-2840-8-9. Cardiovasc Diabetol. 2009. PMID: 19220880 Free PMC article.
-
Long-term efficacy of insulin glargine after switching from NPH insulin as intensive replacement of basal insulin in Japanese diabetes mellitus. Comparison of efficacy between type 1 and type 2 diabetes (JUN-LAN Study 1.2).Endocr J. 2007 Dec;54(6):975-83. doi: 10.1507/endocrj.k07e-035. Epub 2007 Nov 14. Endocr J. 2007. PMID: 18000343
-
Glargine is superior to neutral protamine Hagedorn for improving glycated haemoglobin and fasting blood glucose levels during intensive insulin therapy.Intern Med J. 2005 Sep;35(9):536-42. doi: 10.1111/j.1445-5994.2005.00902.x. Intern Med J. 2005. PMID: 16105155 Clinical Trial.
-
(Ultra-)long-acting insulin analogues for people with type 1 diabetes mellitus.Cochrane Database Syst Rev. 2021 Mar 4;3(3):CD013498. doi: 10.1002/14651858.CD013498.pub2. Cochrane Database Syst Rev. 2021. PMID: 33662147 Free PMC article.
-
Insulin glargine: a review of its therapeutic use as a long-acting agent for the management of type 1 and 2 diabetes mellitus.Drugs. 2001;61(11):1599-624. doi: 10.2165/00003495-200161110-00007. Drugs. 2001. PMID: 11577797 Review.
Cited by
-
Are analogue insulins superior to human insulin in clinical practice?Curr Diab Rep. 2010 Jun;10(3):176-83. doi: 10.1007/s11892-010-0104-8. Curr Diab Rep. 2010. PMID: 20425580
-
The Comparative Dosing and Glycemic Control of Intermediate and Long-Acting Insulins in Adult Patients With Type 1 and 2 Diabetes Mellitus.J Pharm Technol. 2022 Feb;38(1):46-53. doi: 10.1177/87551225211055700. Epub 2021 Nov 10. J Pharm Technol. 2022. PMID: 35141727 Free PMC article. Review.
-
A comparison of methods for estimating the temporal change in a continuous variable: Example of HbA1c in patients with diabetes.Pharmacoepidemiol Drug Saf. 2017 Dec;26(12):1474-1482. doi: 10.1002/pds.4273. Epub 2017 Aug 15. Pharmacoepidemiol Drug Saf. 2017. PMID: 28812323 Free PMC article.
-
Clinical experience with insulin glargine in type 1 diabetes.Diabetes Technol Ther. 2010 Nov;12(11):835-46. doi: 10.1089/dia.2010.0135. Epub 2010 Oct 22. Diabetes Technol Ther. 2010. PMID: 20969435 Free PMC article. Review.
-
Metabolic effects of Basal or premixed insulin treatment in 5077 insulin-naïve type 2 diabetes patients: registry-based observational study in clinical practice.Diabetes Ther. 2014 Jun;5(1):243-54. doi: 10.1007/s13300-014-0068-9. Epub 2014 May 15. Diabetes Ther. 2014. PMID: 24828137 Free PMC article.
References
-
- UK Prospective Diabetes Study Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837–853. doi: 10.1016/S0140-6736(98)07019-6. - DOI - PubMed
-
- National Institute for Health and Clinical Excellence . (Clinical guideline 66) London: NICE; 2008. The management of type 2 diabetes (update)http://www.nice.org.uk/Guidance/CG66
-
- National Institute for Health and Clinical Excellence . (Clinical guideline 15) London: NICE; 2004. Diagnosis and management of type 1 diabetes in children, young people and adults.http://www.nice.org.uk/guidance/index.jsp?action=byID&o=10944
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
