

Mechanical ventilation using non-injurious ventilation settings causes lung injury in the absence of pre-existing lung injury in healthy mice
- PMID: 19152704
- PMCID: PMC2688111
- DOI: 10.1186/cc7688
Mechanical ventilation using non-injurious ventilation settings causes lung injury in the absence of pre-existing lung injury in healthy mice
Abstract
Introduction: Mechanical ventilation (MV) may cause ventilator-induced lung injury (VILI). Present models of VILI use exceptionally large tidal volumes, causing gross lung injury and haemodynamic shock. In addition, animals are ventilated for a relative short period of time and only after a 'priming' pulmonary insult. Finally, it is uncertain whether metabolic acidosis, which frequently develops in models of VILI, should be prevented. To study VILI in healthy mice, the authors used a MV model with clinically relevant ventilator settings, avoiding massive damage of lung structures and shock, and preventing metabolic acidosis.
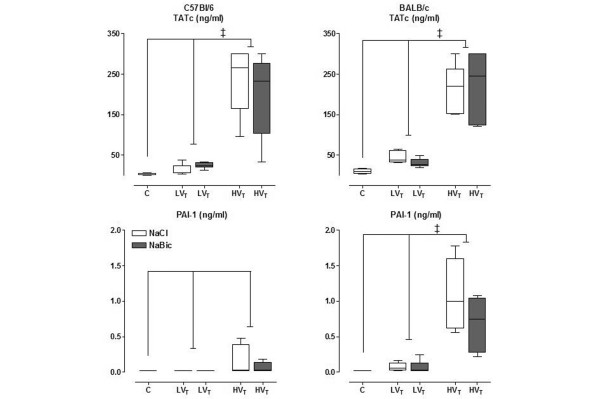
Methods: Healthy C57Bl/6 mice (n = 66) or BALB/c mice (n = 66) were ventilated (tidal volume = 7.5 ml/kg or 15 ml/kg; positive end-expiratory pressure = 2 cmH2O; fraction of inspired oxygen = 0.5) for five hours. Normal saline or sodium bicarbonate were used to correct for hypovolaemia. Lung histopathology, lung wet-to-dry ratio, bronchoalveolar lavage fluid protein content, neutrophil influx and levels of proinflammatory cytokines and coagulation factors were measured.
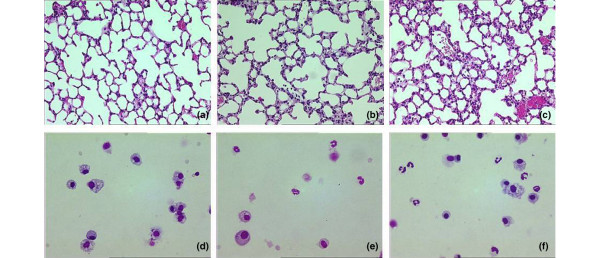
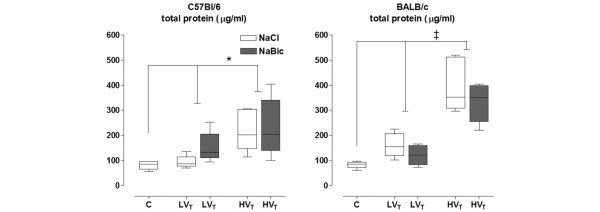
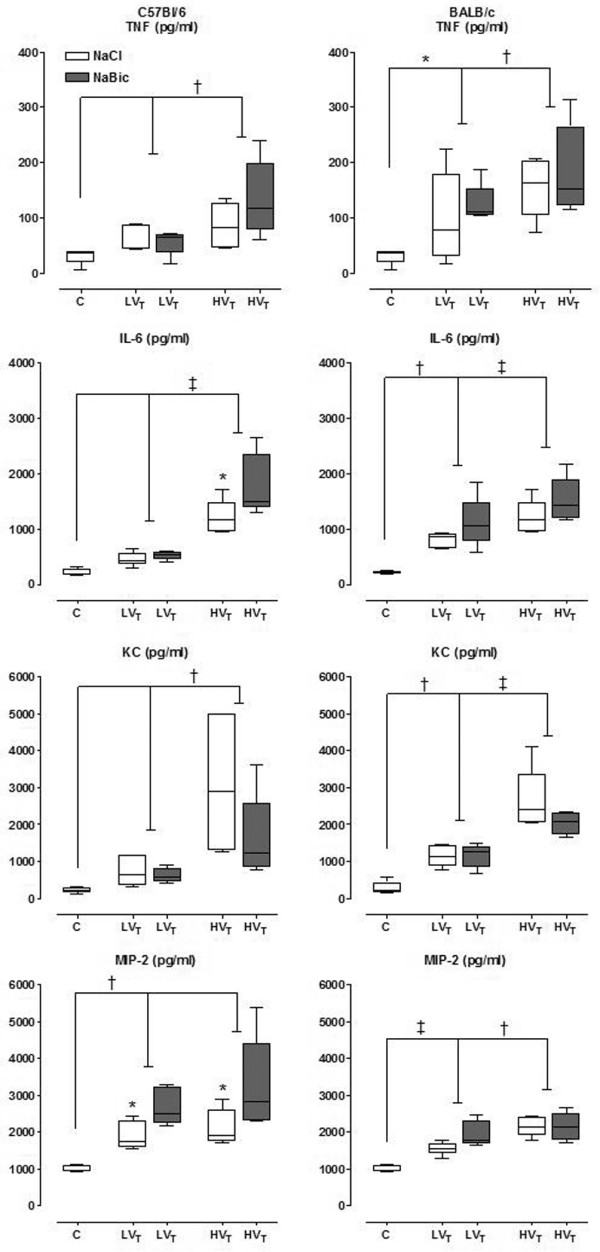
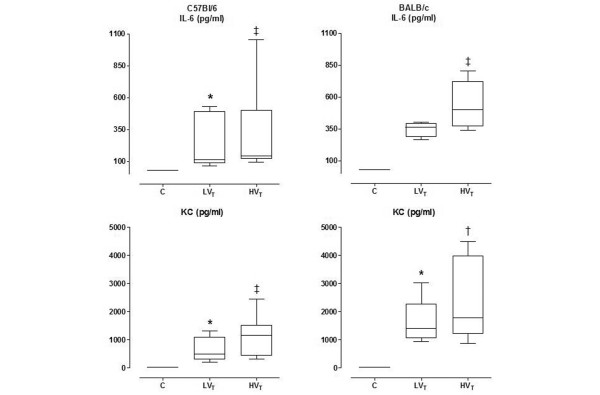
Results: Animals remained haemodynamically stable throughout the whole experiment. Lung histopathological changes were minor, although significantly more histopathological changes were found after five hours of MV with a larger tidal volume. Lung histopathological changes were no different between the strains. In both strains and with both ventilator settings, MV caused higher wet-to-dry ratios, higher bronchoalveolar lavage fluid protein levels and more influx of neutrophils, and higher levels of proinflammatory cytokines and coagulation factors. Also, with MV higher systemic levels of cytokines were measured. All parameters were higher with larger tidal volumes. Correcting for metabolic acidosis did not alter endpoints.
Conclusions: MV induces VILI, in the absence of a priming pulmonary insult and even with use of relevant (least injurious) ventilator settings. This model offers opportunities to study the pathophysiological mechanisms behind VILI and the contribution of MV to lung injury in the absence of pre-existing lung injury.
Figures
Comment in
-
Gene expression changes with a 'non-injurious' ventilation strategy.Crit Care. 2009;13(2):403. doi: 10.1186/cc7719. Epub 2009 Mar 4. Crit Care. 2009. PMID: 19291277 Free PMC article. No abstract available.
References
-
- Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858–873. doi: 10.1097/01.CCM.0000117317.18092.E4. - DOI - PubMed
-
- Wilson MR, Choudhury S, Goddard ME, O'Dea KP, Nicholson AG, Takata M. High tidal volume upregulates intrapulmonary cytokines in an in vivo mouse model of ventilator-induced lung injury. J Appl Physiol. 2003;95:1385–1393. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
