

Avoiding hospital admission through provision of hospital care at home: a systematic review and meta-analysis of individual patient data
- PMID: 19153394
- PMCID: PMC2621299
- DOI: 10.1503/cmaj.081491
Avoiding hospital admission through provision of hospital care at home: a systematic review and meta-analysis of individual patient data
Abstract
Background: Avoidance of admission through provision of hospital care at home is a scheme whereby health care professionals provide active treatment in the patient's home for a condition that would otherwise require inpatient treatment in an acute care hospital. We sought to compare the effectiveness of this method of caring for patients with that type of in-hospital care.
Methods: We searched the MEDLINE, EMBASE, CINAHL and EconLit databases and the Cochrane Effective Practice and Organisation of Care Group register from the earliest date in each database until January 2008. We included randomized controlled trials that evaluated a service providing an alternative to admission to an acute care hospital. We excluded trials in which the program did not offer a substitute for inpatient care. We performed meta-analyses for trials for which the study populations had similar characteristics and for which common outcomes had been measured.
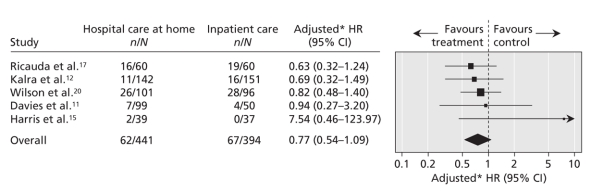
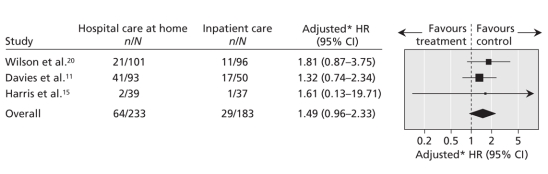
Results: We included 10 randomized trials (with a total of 1327 patients) in our systematic review. Seven of these trials (with a total of 969 patients) were deemed eligible for meta-analysis of individual patient data, but we were able to obtain data for only 5 of these trials (with a total of 844 patients [87%]). There was no significant difference in mortality at 3 months for patients who received hospital care at home (adjusted hazard ratio [HR] 0.77, 95% confidence interval [CI] 0.54-1.09, p = 0.15). However, at 6 months, mortality was significantly lower for these patients (adjusted HR 0.62, 95% CI 0.45-0.87, p = 0.005). Admissions to hospital were greater, but not significantly so, for patients receiving hospital care at home (adjusted HR 1.49, 95% CI 0.96-2.33, p = 0.08). Patients receiving hospital care at home reported greater satisfaction than those receiving inpatient care. These programs were less expensive than admission to an acute care hospital ward when the analysis was restricted to treatment actually received and when the costs of informal care were excluded.
Interpretation: For selected patients, avoiding admission through provision of hospital care at home yielded similar outcomes to inpatient care, at a similar or lower cost.
Figures


Comment in
-
Defining and disseminating the hospital-at-home model.CMAJ. 2009 Jan 20;180(2):156-7. doi: 10.1503/cmaj.081891. CMAJ. 2009. PMID: 19153385 Free PMC article. No abstract available.
References
-
- Parker G, Bhakta P, Lovett CA, et al. A systematic review of the costs and effectiveness of different models of paediatric home care. Health Technol Assess 2002;6:iii-108. - PubMed
-
- Wolfe CDA, Tilling K, Rudd AG. The effectiveness of community based rehabilitation for stroke patients who remain at home: a pilot randomised trial. Clin Rehabil 2000;14:563-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases