

Antiviral prophylaxis during pandemic influenza may increase drug resistance
- PMID: 19154598
- PMCID: PMC2654456
- DOI: 10.1186/1471-2334-9-4
Antiviral prophylaxis during pandemic influenza may increase drug resistance
Abstract
Background: Neuraminidase inhibitors (NI) and social distancing play a major role in plans to mitigate future influenza pandemics.
Methods: Using the freely available program InfluSim, the authors examine to what extent NI-treatment and prophylaxis promote the occurrence and transmission of a NI resistant strain.
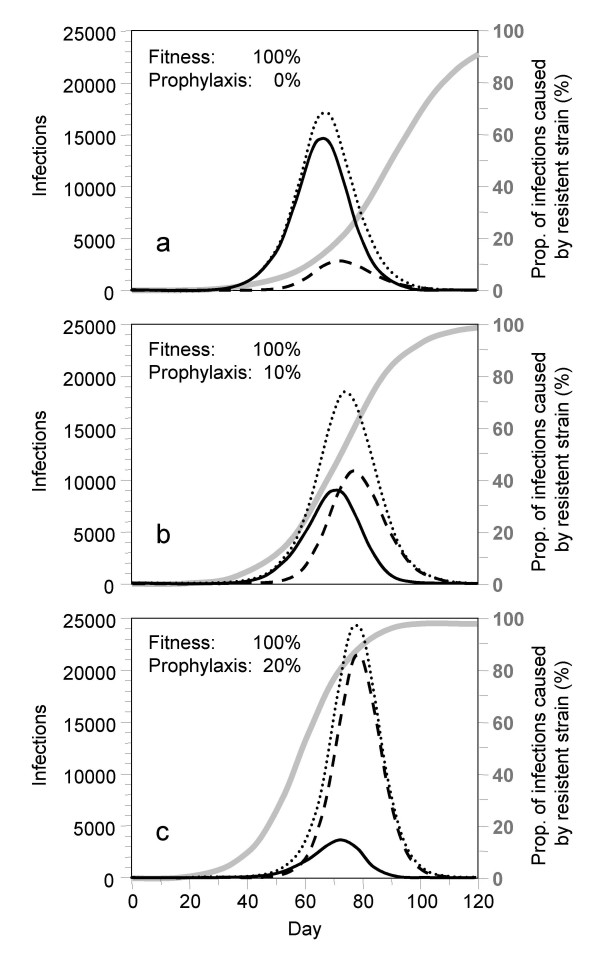
Results: Under a basic reproduction number of R0 = 2.5, a NI resistant strain can only spread if its transmissibility (fitness) is at least 40% of the fitness of the drug-sensitive strain. Although NI drug resistance may emerge in treated patients in such a late state of their disease that passing on the newly developed resistant viruses is unlikely, resistant strains quickly become highly prevalent in the population if their fitness is high. Antiviral prophylaxis further increases the pressure on the drug-sensitive strain and favors the spread of resistant infections. The authors show scenarios where pre-exposure antiviral prophylaxis even increases the number of influenza cases and deaths.
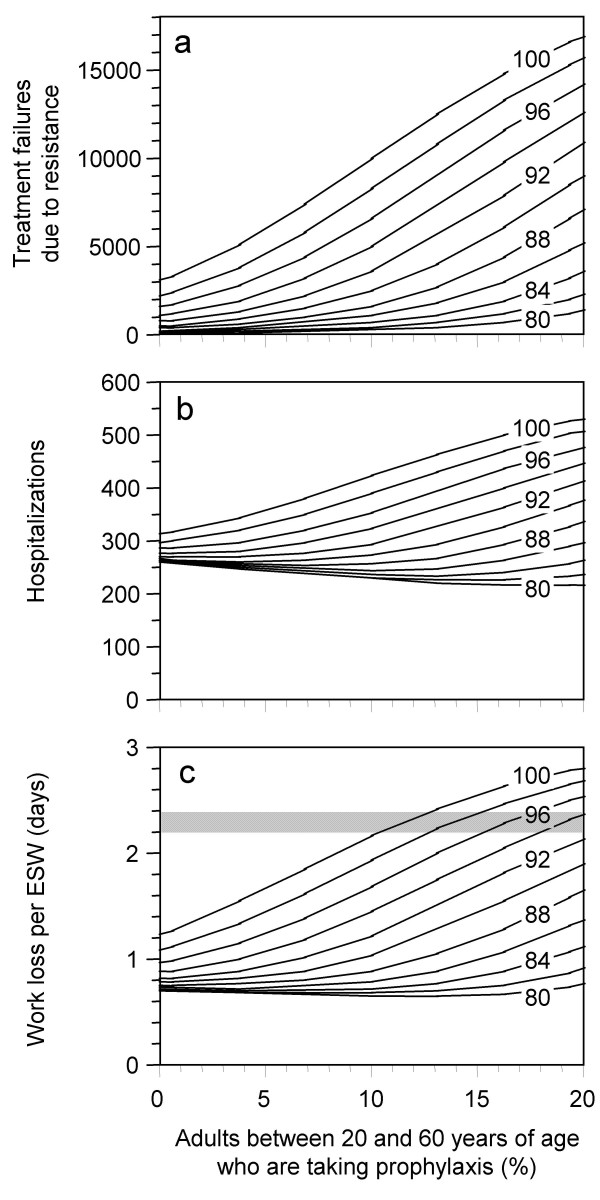
Conclusion: If the fitness of a NI resistant pandemic strain is high, any use of prophylaxis may increase the number of hospitalizations and deaths in the population. The use of neuraminidase inhibitors should be restricted to the treatment of cases whereas prophylaxis should be reduced to an absolute minimum in that case.
Figures
Similar articles
-
Modeling the effects of drug resistant influenza virus in a pandemic.Virol J. 2008 Oct 30;5:133. doi: 10.1186/1743-422X-5-133. Virol J. 2008. PMID: 18973656 Free PMC article.
-
Antiviral resistance and the control of pandemic influenza.PLoS Med. 2007 Jan;4(1):e15. doi: 10.1371/journal.pmed.0040015. PLoS Med. 2007. PMID: 17253900 Free PMC article.
-
Use of neuraminidase inhibitors to combat pandemic influenza.J Antimicrob Chemother. 2006 Nov;58(5):911-5. doi: 10.1093/jac/dkl376. Epub 2006 Sep 6. J Antimicrob Chemother. 2006. PMID: 16956904
-
Neuraminidase inhibitor resistance in influenza viruses and laboratory testing methods.Antivir Ther. 2012;17(1 Pt B):159-73. doi: 10.3851/IMP2067. Epub 2012 Feb 3. Antivir Ther. 2012. PMID: 22311680 Review.
-
Neuraminidase inhibitors and their role in avian and pandemic influenza.Antivir Ther. 2007;12(4 Pt B):593-602. Antivir Ther. 2007. PMID: 17944267 Review.
Cited by
-
Developing guidelines for school closure interventions to be used during a future influenza pandemic.BMC Infect Dis. 2010 Jul 27;10:221. doi: 10.1186/1471-2334-10-221. BMC Infect Dis. 2010. PMID: 20659348 Free PMC article.
-
Pandemic Influenza A H1N1 (2009) Virus: Lessons from the Past and Implications for the Future.Indian J Virol. 2012 Jun;23(1):12-7. doi: 10.1007/s13337-012-0066-3. Epub 2012 Mar 25. Indian J Virol. 2012. PMID: 23729996 Free PMC article.
-
Assessing the oseltamivir-induced resistance risk and implications for influenza infection control strategies.Infect Drug Resist. 2017 Jul 20;10:215-226. doi: 10.2147/IDR.S138317. eCollection 2017. Infect Drug Resist. 2017. PMID: 28790857 Free PMC article.
-
Emergency Medical Services Personnel's Pandemic Influenza Training Received and Willingness to Work during a Future Pandemic.Prehosp Emerg Care. 2020 Sep-Oct;24(5):601-609. doi: 10.1080/10903127.2019.1701158. Epub 2020 Jan 7. Prehosp Emerg Care. 2020. PMID: 31800338 Free PMC article.
-
Tracking oseltamivir-resistance in New Zealand influenza viruses during a medicine reclassification in 2007, a resistant-virus importation in 2008 and the 2009 pandemic.Western Pac Surveill Response J. 2012 Oct 30;3(4):71-7. doi: 10.5365/WPSAR.2012.3.3.002. Print 2012 Oct. Western Pac Surveill Response J. 2012. PMID: 23908945 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
