

The effect of volume on esophageal cancer resections: what constitutes acceptable resection volumes for centers of excellence?
- PMID: 19154895
- PMCID: PMC2631576
- DOI: 10.1016/j.jtcvs.2008.09.040
The effect of volume on esophageal cancer resections: what constitutes acceptable resection volumes for centers of excellence?
Abstract
Objective: Volume-outcome relationships for esophageal cancer resection have been well described with centers of excellence defined by volume. No consensus exists for what constitutes a "high-volume" center. We aim to determine if an objective evidence-based threshold of operative volume associated with improvement in operative outcome for esophageal resections can be defined.
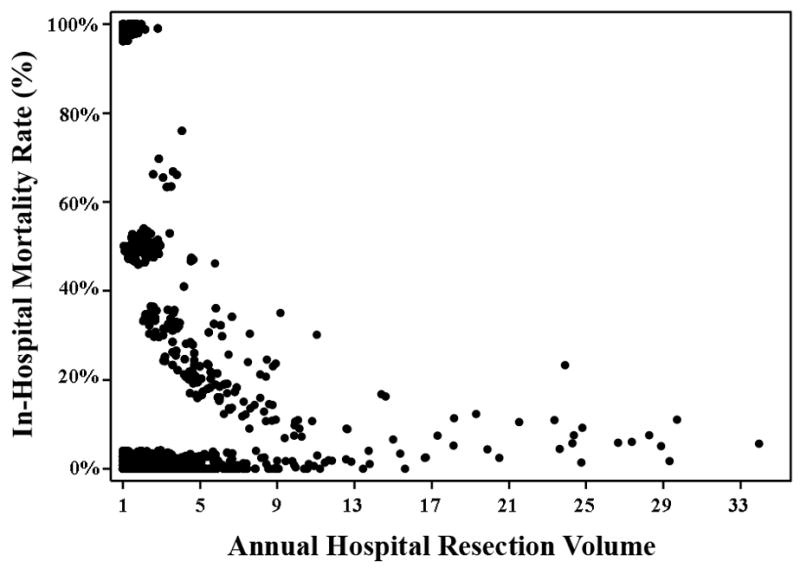
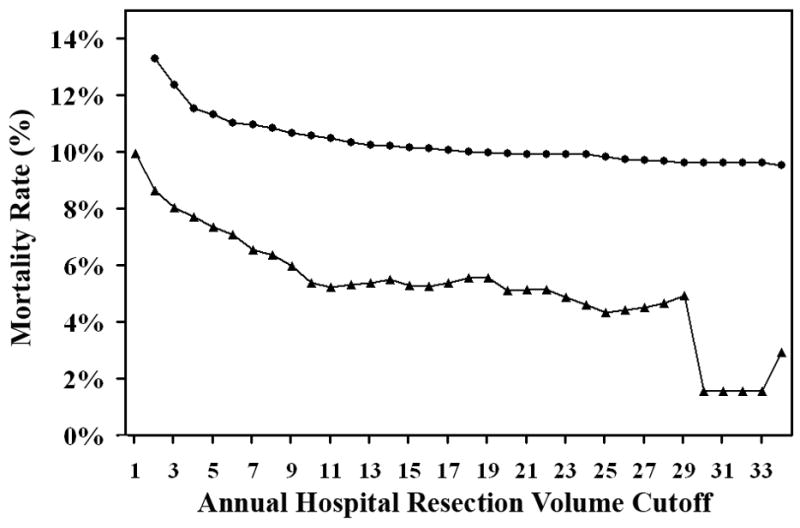
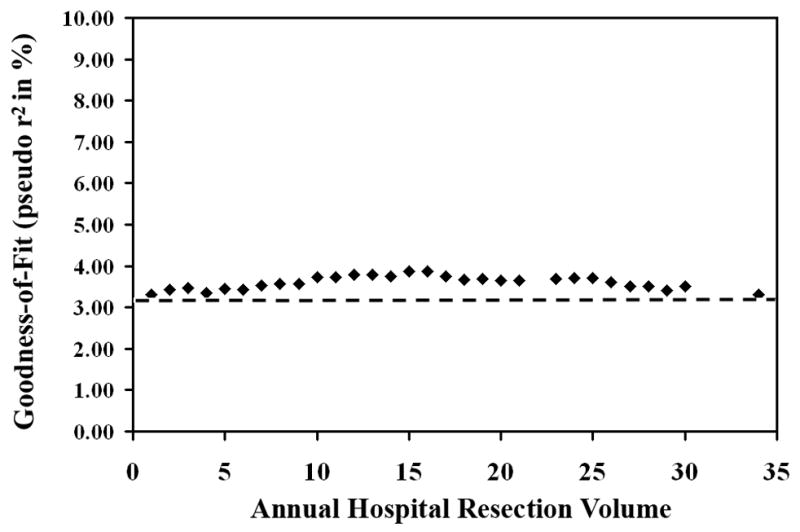
Methods: Retrospective analysis was performed on patients undergoing esophageal resection for cancer in the 1998 to 2005 Nationwide Inpatient Sample. A series of multivariable analyses were performed, changing the resection volume cutoff to account for the range of annual hospital resections. The goodness of fit of each model was compared by pseudo r(2), the amount of data variance explained by each model.
Results: A total of 4080 patients underwent esophageal resection. The median annual hospital resection volume was 4 (range: 1-34). The mortality rate of "high-volume" centers ranged from 9.94% (>or=2 resection/year) to 1.56% (>or=30 resections/year). The best model was with an annual hospital resection volume greater than or equal to 15 (3.87% of data variance explained). The difference in goodness of fit between the best model and other models with different volume cutoffs was 0.64%, suggesting that volume explains less than 1% of variance in perioperative death.
Conclusion: Our data do not support the use of volume cutoffs for defining centers of excellence for esophageal cancer resections. Although volume has an incremental impact on mortality, volume alone is insufficient for defining centers of excellence. Volume seems to function as an imperfect surrogate for other variables, which may better define centers of excellence. Additional work is needed to identify these variables.
Figures
Comment in
-
Esophagectomy volume threshold as a criterion for centers of excellence: causation or cause, strategy or strategem?J Thorac Cardiovasc Surg. 2009 Jan;137(1):10-2. doi: 10.1016/j.jtcvs.2008.06.041. J Thorac Cardiovasc Surg. 2009. PMID: 19154892 No abstract available.
References
-
- Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relation between surgical volume and mortality. N Engl J Med. 1979;301:1364–1369. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital volume on operative mortality for major cancer surgery. Jama. 1998;280:1747–1751. - PubMed
-
- Dimick JB, Cattaneo SM, Lipsett PA, Pronovost PJ, Heitmiller RF. Hospital volume is related to clinical and economic outcomes of esophageal resection in Maryland. Ann Thorac Surg. 2001;72:334–339. discussion 339-341. - PubMed
-
- Kuo EY, Chang Y, Wright CD. Impact of hospital volume on clinical and economic outcomes for esophagectomy. Ann Thorac Surg. 2001;72:1118–1124. - PubMed
-
-
Leapfrog Group “Evidence-based hospital referral” for esophageal cancer. 2003: leapfroggroup.org, accessioned Nov 21, 2006.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
