

Prediction of fatal or near-fatal cardiac arrhythmia events in patients with depressed left ventricular function after an acute myocardial infarction
- PMID: 19155249
- PMCID: PMC2655314
- DOI: 10.1093/eurheartj/ehn537
Prediction of fatal or near-fatal cardiac arrhythmia events in patients with depressed left ventricular function after an acute myocardial infarction
Abstract
Aims: To determine whether risk stratification tests can predict serious arrhythmic events after acute myocardial infarction (AMI) in patients with reduced left ventricular ejection fraction (LVEF < or = 0.40).
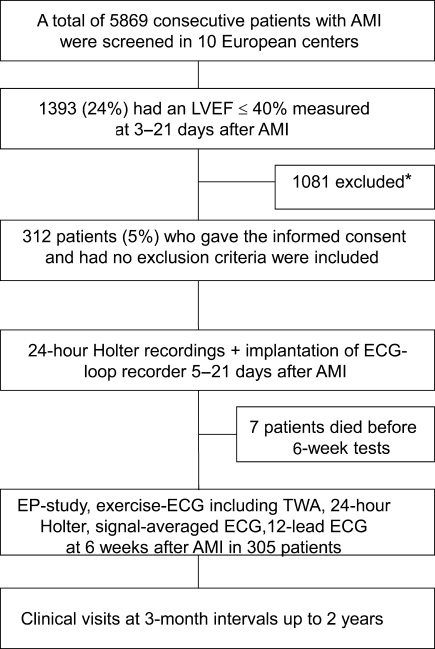
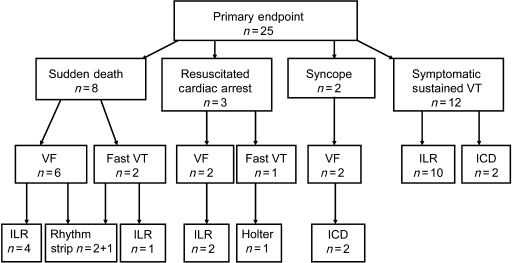
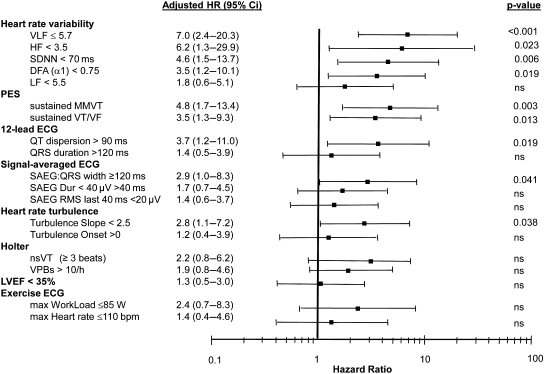
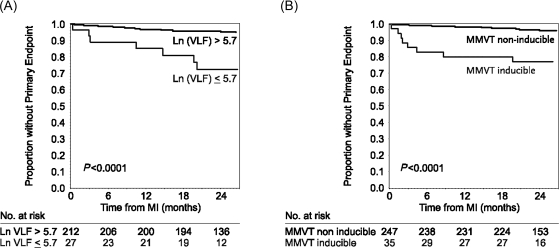
Methods and results: A total of 5869 consecutive patients were screened in 10 European centres, and 312 patients (age 65 +/- 11 years) with a mean LVEF of 31 +/- 6% were included in the study. Heart rate variability/turbulence, ambient arrhythmias, signal-averaged electrocardiogram (SAECG), T-wave alternans, and programmed electrical stimulation (PES) were performed 6 weeks after AMI. The primary endpoint was ECG-documented ventricular fibrillation or symptomatic sustained ventricular tachycardia (VT). To document these arrhythmic events, the patients received an implantable ECG loop-recorder. There were 25 primary endpoints (8.0%) during the follow-up of 2 years. The strongest predictors of primary endpoint were measures of heart rate variability, e.g. hazard ratio (HR) for reduced very-low frequency component (<5.7 ln ms(2)) adjusted for clinical variables was 7.0 (95% CI: 2.4-20.3, P < 0.001). Induction of sustained monomorphic VT during PES (adjusted HR = 4.8, 95% CI, 1.7-13.4, P = 0.003) also predicted the primary endpoint.
Conclusion: Fatal or near-fatal arrhythmias can be predicted by many risk stratification methods, especially by heart rate variability, in patients with reduced LVEF after AMI.
Trial registration: ClinicalTrials.gov NCT00145119.
Figures
Comment in
-
Prediction of fatal or near fatal arrhythmias in patients with a depressed left ventricular function after an acute myocardial infarction.Eur Heart J. 2009 May;30(10):1288. doi: 10.1093/eurheartj/ehp166. Epub 2009 Apr 20. Eur Heart J. 2009. PMID: 19380348 No abstract available.
References
-
- Camm AJ, Pratt CM, Schwartz PJ, Al-Khalidi HR, Spyt MJ, Holroyde MJ, Karam R, Sonnenblick EH, Brum JM AzimiLide post Infarct surVival Evaluation (ALIVE) Investigators. Mortality in patients after a recent myocardial infarction: a randomized, placebo-controlled trial of azimilide using heart rate variability for risk stratification. Circulation. 2004;109:990–996. - PubMed
-
- Solomon SD, Zelenkofske S, McMurray JJ, Finn PV, Velazquez E, Ertl G, Harsanyi A, Rouleau JL, Maggioni A, Kober L, White H, Van de Werf F, Pieper K, Califf RM, Pfeffer MA Valsartan in Acute Myocardial Infarction Trial (VALIANT) Investigators. Sudden death in patients with myocardial infarction and left ventricular dysfunction, heart failure, or both. N Engl J Med. 2005;352:2581–2588. - PubMed
-
- Hohnloser SH, Kuck KH, Dorian P, Roberts RS, Hampton JR, Hatala R, Fain E, Gent M, Connolly SJ DINAMIT Investigators. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004;351:2481–2488. - PubMed
-
- Huikuri HV, Castellanos A, Myerburg RJ. Sudden death due to cardiac arrhythmias. N Engl J Med. 2001;345:1473–1482. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–883. - PubMed
