

Left ventricular function and exercise capacity
- PMID: 19155455
- PMCID: PMC2862454
- DOI: 10.1001/jama.2008.1022
Left ventricular function and exercise capacity
Abstract
Context: Limited information exists regarding the role of left ventricular function in predicting exercise capacity and impact on age- and sex-related differences.
Objectives: To determine the impact of measures of cardiac function assessed by echocardiography on exercise capacity and to determine if these associations are modified by sex or advancing age.
Design: Cross-sectional study of patients undergoing exercise echocardiography with routine measurements of left ventricular systolic and diastolic function by 2-dimensional and Doppler techniques. Analyses were conducted to determine the strongest correlates of exercise capacity and the age and sex interactions of these variables with exercise capacity.
Setting: Large tertiary referral center in Rochester, Minnesota, in 2006.
Participants: Patients undergoing exercise echocardiography using the Bruce protocol (N = 2867). Patients with echocardiographic evidence of exercise-induced ischemia, ejection fractions lower than 50%, or significant valvular heart disease were excluded.
Main outcome measure: Exercise capacity in metabolic equivalents (METs).
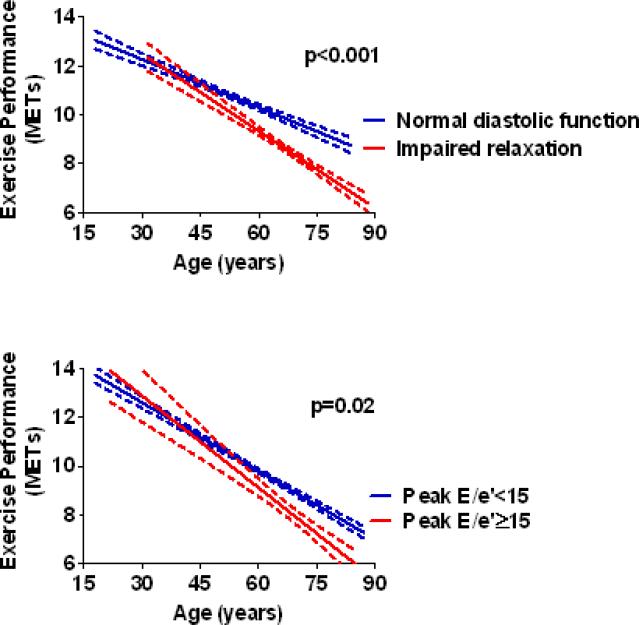
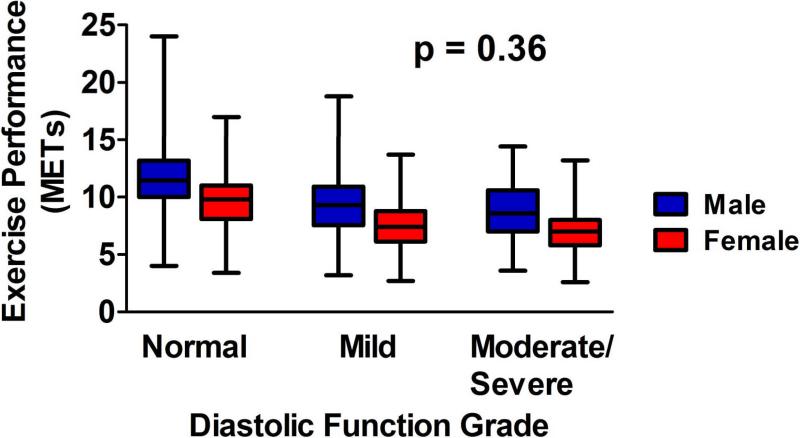
Results: Diastolic dysfunction was strongly and inversely associated with exercise capacity. Compared with normal function, after multivariate adjustment, those with moderate/severe resting diastolic dysfunction (-1.30 METs; 95% confidence interval [CI], -1.52 to -0.99; P < .001) and mild resting diastolic dysfunction (-0.70 METs; 95% CI, -0.88 to -0.46; P < .001) had substantially lower exercise capacity. Variation of left ventricular systolic function within the normal range was not associated with exercise capacity. Left ventricular filling pressures measured by resting E/e' of 15 or greater (-0.41 METs; 95% CI, -0.70 to -0.11; P = .007) or postexercise E/e' of 15 or greater (-0.41 METs; 95% CI, -0.71 to -0.11; P = .007) were similarly associated with a reduction in exercise capacity, each in separate multivariate analyses. Individuals with impaired relaxation (mild dysfunction) or resting E/e' of 15 or greater had a progressive increase in the magnitude of reduction in exercise capacity with advancing age (P < .001 and P = .02, respectively). Other independent correlates of exercise capacity were age (unstandardized beta coefficient, -0.85 METs; 95% CI, -0.92 to -0.77, per 10-year increment; P < .001), female sex (-1.98 METs; 95% CI, -2.15 to -1.84; P < .001), and body mass index greater than 30 (-1.24 METs; 95% CI, -1.41 to -1.10; P < .001).
Conclusion: In this large cross-sectional study of those referred for exercise echocardiography and not limited by ischemia, abnormalities of left ventricular diastolic function were independently associated with exercise capacity.
Figures
Comment in
-
Exercise capacity and left ventricular function.JAMA. 2009 Jun 10;301(22):2325-6; author reply 2326-7. doi: 10.1001/jama.2009.696. JAMA. 2009. PMID: 19509376 No abstract available.
-
Exercise capacity and left ventricular function.JAMA. 2009 Jun 10;301(22):2326; author reply 2326-7. doi: 10.1001/jama.2009.697. JAMA. 2009. PMID: 19509377 No abstract available.
References
-
- Woo JS, Derleth C, Stratton JR, Levy WC. The Influence of Age, Gender, and Training on Exercise Efficiency. J Am Coll Cardiol. 2006;47(5):1049–1057. - PubMed
-
- Hossack KF, Bruce RA. Maximal cardiac function in sedentary normal men and women: comparison of age-related changes. J Appl Physiol. 1982;53(4):799–804. - PubMed
-
- Weiss EP, Spina RJ, Holloszy JO, Ehsani AA. Gender differences in the decline in aerobic capacity and its physiological determinants during the later decades of life. J Appl Physiol. 2006;101(3):938–944. - PubMed
-
- Shubair MM, Kodis J, McKelvie RS. Metabolic profile and exercise capacity outcomes: their relationship to overweight and obesity in a Canadian rehabilitation setting. J Cardiopulm Rehabil. 2004;24(6):405–413. - PubMed
-
- Enright PL, McBurnie MA, Bittner V, et al. The 6-min walk test: a quick measure of functional status in elderly adults. Chest. 2003;123(2):387–398. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
