

Diagnostic performance of fusion of myocardial perfusion imaging (MPI) and computed tomography coronary angiography
- PMID: 19156478
- PMCID: PMC3086676
- DOI: 10.1007/s12350-008-9019-z
Diagnostic performance of fusion of myocardial perfusion imaging (MPI) and computed tomography coronary angiography
Abstract
Background: We evaluated the incremental diagnostic value of fusion images of coronary computed tomography angiography (CTA) and myocardial perfusion imaging (MPI) over MPI alone or MPI and CTA side-by-side to identify obstructive coronary artery disease (CAD > 50% stenosis) using invasive coronary angiography (ICA) as the gold standard.
Methods: 50 subjects (36 men; 56 +/- 11 years old) underwent rest-stress MPI and CTA within 12-26 days of each other. CTAs were performed with multi-detector CT-scanners (31 on 64-slice; and 19 on 16-slice). 37 patients underwent ICA while 13 subjects did not because of low (<5%) pre-test likelihood (LLK) of disease. Three blinded readers scored the images in sequential sessions using (1) MPI alone (2) MPI and CTA side-by-side, (3) fused CTA/MPI images.
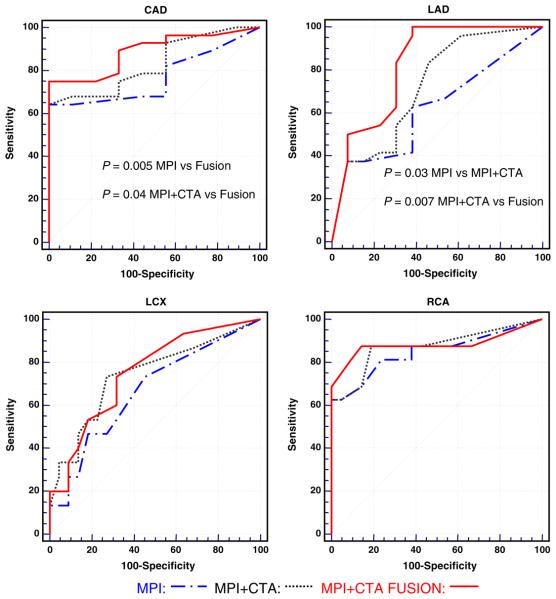
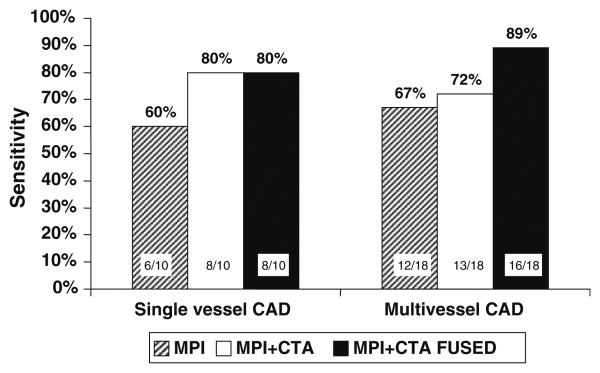
Results: One or more critical stenoses during ICA were found in 28 patients and non-critical stenoses were found in 9 patients. MPI, side-by-side MPI-CTA, and fused CTA/MPI showed the same normalcy rate (NR:13/13) in LLK subjects. The fusion technique performed better than MPI and MPI and CTA side-by-side for the presence of CAD in any vessel (overall area under the curve (AUC) for fused images: 0.89; P = .005 vs MPI, P = .04 vs side-by-side MPI-CTA) and for localization of CAD to the left anterior descending coronary artery (AUC: 0.82, P < .001 vs MPI; P = .007 vs side-by-side MPI-CTA). There was a non-significant trend for better detection of multi-vessel disease with fusion.
Conclusions: Using ICA as the gold standard, fusion imaging provided incremental diagnostic information compared to MPI alone or side-by-side MPI-CTA for the diagnosis of obstructive CAD and for localization of CAD to the left anterior descending coronary artery.
Figures
Comment in
-
Combining CT and nuclear: a winning hybrid team.J Nucl Cardiol. 2009 Mar-Apr;16(2):170-2. doi: 10.1007/s12350-008-9048-7. Epub 2009 Jan 6. J Nucl Cardiol. 2009. PMID: 19127395 No abstract available.
References
-
- Shaw LJ, Shaw RE, Merz CN, et al. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry. Circulation. 2008;117:1787–801. - PubMed
-
- Schoepf UJ, Becker CR, Ohnesorge BM, Yucel EK. CT of coronary artery disease. Radiology. 2004;232:18–37. - PubMed
-
- Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med. 1979;300:1350–8. - PubMed
-
- Grossman GB, Garcia EV, Bateman TM, et al. Quantitative Tc-99m sestamibi attenuation-corrected SPECT: development and multicenter trial validation of myocardial perfusion stress gender-independent normal database in an obese population. J Nucl Cardiol. 2004;11:263–72. - PubMed
-
- Case JAPT, O'Brian-Penny B, King MA, Luo DS, Rabin MSZ. Reduction of truncation artifacts in fan beam transmission imaging using a spatially varying gamma prior. IEEE-TNS. 1995;42:1310–20.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
