

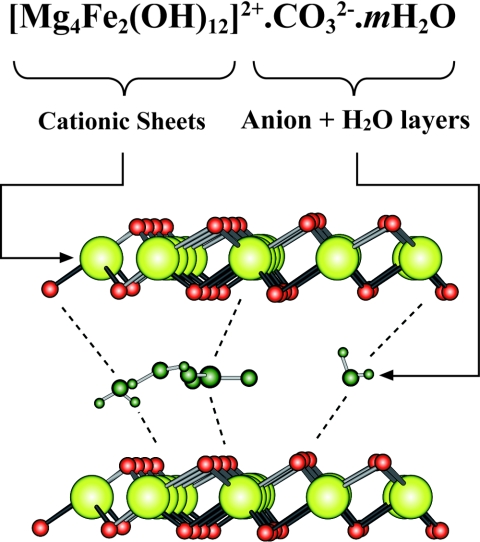
Iron-magnesium hydroxycarbonate (fermagate): a novel non-calcium-containing phosphate binder for the treatment of hyperphosphatemia in chronic hemodialysis patients
- PMID: 19158369
- PMCID: PMC2637599
- DOI: 10.2215/CJN.02630608
Iron-magnesium hydroxycarbonate (fermagate): a novel non-calcium-containing phosphate binder for the treatment of hyperphosphatemia in chronic hemodialysis patients
Abstract
Background and objectives: This phase II study tested the safety and efficacy of fermagate, a calcium-free iron and magnesium hydroxycarbonate binder, for treating hyperphosphatemia in hemodialysis patients.
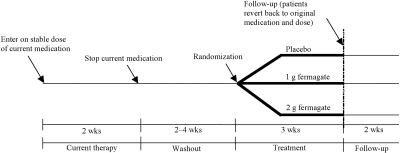
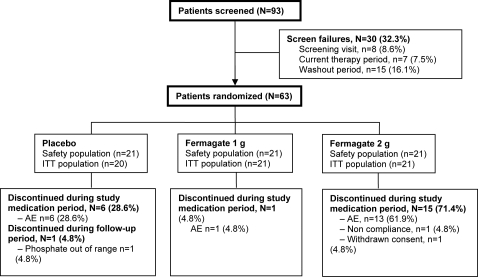
Design, setting, participants, & measurements: A randomized, double-blind, three-arm, parallel-group study compared two doses of fermagate (1 g three times daily or 2 g three times daily with placebo). Sixty-three patients who had been on a stable hemodialysis regimen for > or =3 mo were randomized to the treatment phase. Study medication was administered three times daily just before meals for 21 d. The primary endpoint was reduction in serum phosphate over this period.
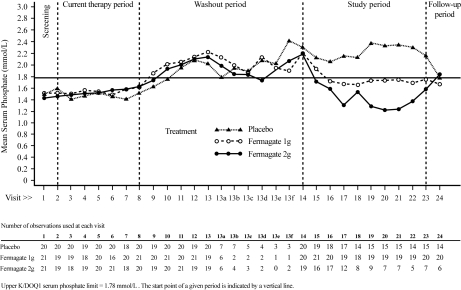
Results: In the intention-to-treat analysis, mean baseline serum phosphate was 2.16 mmol/L. The fermagate 1- and 2-g three-times-daily treatment arms were associated with statistical reductions in mean serum phosphate to 1.71 and 1.47 mmol/L, respectively. Adverse event (AE) incidence in the 1-g fermagate arm was statistically comparable to the placebo group. The 2-g arm was associated with a statistically higher number of patients reporting AEs than the 1-g arm, particularly gastrointestinal AEs, as well as a higher number of discontinuations, complicating interpretation of this dose's efficacy. Both doses were associated with elevations of prehemodialysis serum magnesium levels.
Conclusions: The efficacy and tolerability of fermagate were dose dependent. Fermagate showed promising efficacy in the treatment of hyperphosphatemia in chronic hemodialysis patients as compared with placebo in this initial phase II study. The optimal balance between efficacy and tolerability needs to be determined from future dose-titration studies, or fixed-dose comparisons of more doses.
Figures
References
-
- Gipstein RM, Coburn JW, Adams DA, Lee DB, Parsa KP, Sellers A, Suki WN, Massry SG: Calciphylaxis in man. A syndrome of tissue necrosis and vascular calcification in 11 patients with chronic renal failure. Arch Intern Med 136: 1273–1280, 1976 - PubMed
-
- Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB: Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 342: 1478–1483, 2000 - PubMed
-
- Janigan DT, Hirsch DJ, Klassen GA, MacDonald AS: Calcified subcutaneous arterioles with infarcts of the subcutis and skin (“calciphylaxis”) in chronic renal failure. Am J Kidney Dis 35: 588–597, 2000 - PubMed
-
- London GM, Guerin AP, Marchais SJ, Metivier F, Pannier B, Adda H: Arterial media calcification in end-stage renal disease: Impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant 18: 1731–1740, 2003 - PubMed
-
- Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM: Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol 15: 2208–2218, 2004 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
