

10-year trends in the diagnosis and treatment of hepatitis C and concomitant mental health disorders: 1995 to 2005
- PMID: 19158972
- PMCID: PMC2629062
- DOI: 10.4088/pcc.v10n0501
10-year trends in the diagnosis and treatment of hepatitis C and concomitant mental health disorders: 1995 to 2005
Abstract
Objective: To evaluate trends in the rate and timing of treatment for hepatitis C in those with and without mental health comorbidities.
Method: Data from the population-based Olmsted County Hepatitis C Registry in Minnesota were linked to patients' medical records to identify the dates and duration of any hepatitis C-specific therapy as well as all diagnoses of mental health comorbid conditions prior to initiation of therapy. The most common mental health conditions, major depressive disorder, alcohol dependence, and intravenous drug use, were assessed separately. The registry includes all Olmsted County residents with a physician diagnosis of hepatitis C or non-A/non-B hepatitis (ICD-9 criteria) from January 1, 1990, through December 31, 2005.
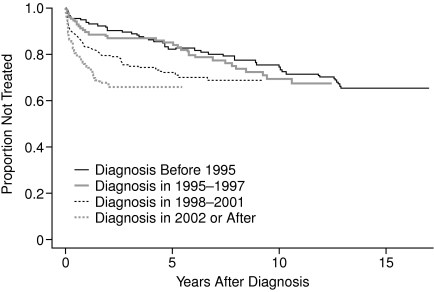
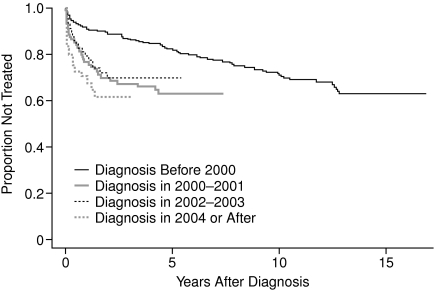
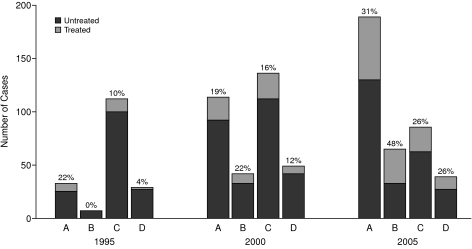
Results: The age-adjusted prevalence of diagnosed hepatitis C increased markedly between 1995 and 2000 (15.5/10,000 persons to 27.0/10,000 persons) but changed little between 2000 and 2005 (27.0 to 27.9/10,000 persons). The number of people with comorbid hepatitis C and depressive disorder (including minor depression) increased significantly between 1995 and 2005 from 18% to over 35% of all people with diagnosed hepatitis C. Treatment rates more than doubled between 1995 and 2005, while the time from diagnosis to treatment decreased during that same period. By 2005, major depressive disorders were associated with a high rate of reasonably prompt treatment. There were no gender differences in treatment rates or time to treatment when other comorbidities and age were included in the analyses.
Conclusions: From 1995 to 2005, rates of treatment for hepatitis C among people with and without comorbid mental health problems increased. Rates of increase were higher among those with depression and hepatitis C than among those with hepatitis C and drug abuse or other mental health diagnoses. Even with this progress in treating those with multiple diagnoses, over 75% of people with hepatitis C remain untreated.
Figures

Similar articles
-
Development and maintenance of a community-based hepatitis C registry.Am J Manag Care. 2002 Mar;8(3):253-61. Am J Manag Care. 2002. PMID: 11915975
-
Psychiatric Diagnoses and Comorbidities in a Diverse, Multicity Cohort of Young Transgender Women: Baseline Findings From Project LifeSkills.JAMA Pediatr. 2016 May 1;170(5):481-6. doi: 10.1001/jamapediatrics.2016.0067. JAMA Pediatr. 2016. PMID: 26999485 Free PMC article.
-
Diagnoses of sexual abuse and their common registered comorbidities in the total population of Stockholm.J Epidemiol Community Health. 2017 Jun;71(6):592-598. doi: 10.1136/jech-2016-208105. Epub 2017 Jan 11. J Epidemiol Community Health. 2017. PMID: 28077602
-
Interventions for adults with a history of complex traumatic events: the INCiTE mixed-methods systematic review.Health Technol Assess. 2020 Sep;24(43):1-312. doi: 10.3310/hta24430. Health Technol Assess. 2020. PMID: 32924926 Free PMC article.
-
[Hepatitis C, interferon a and depression: main physiopathologic hypothesis].Encephale. 2005 May-Jun;31(3):349-57. doi: 10.1016/s0013-7006(05)82400-5. Encephale. 2005. PMID: 16142050 Review. French.
Cited by
-
Health-related quality of life (HRQL) for individuals with self-reported chronic physical and/or mental health conditions: panel survey of an adult sample in the United States.Health Qual Life Outcomes. 2012 Dec 19;10:154. doi: 10.1186/1477-7525-10-154. Health Qual Life Outcomes. 2012. PMID: 23253258 Free PMC article.
-
Context of clinical care: the case of hepatitis C in underserved communities--a report from the Primary Care Multiethnic Network (PRIME Net) Consortium.J Am Board Fam Med. 2009 Nov-Dec;22(6):638-46. doi: 10.3122/jabfm.2009.06.090020. J Am Board Fam Med. 2009. PMID: 19897692 Free PMC article.
-
Treatment of psychological co-morbidities in common gastrointestinal and hepatologic disorders.World J Gastrointest Pharmacol Ther. 2010 Apr 6;1(2):64-71. doi: 10.4292/wjgpt.v1.i2.64. World J Gastrointest Pharmacol Ther. 2010. PMID: 21577298 Free PMC article.
-
Increase in nonhepatic diagnoses among persons with hepatitis C hospitalized for any cause, United States, 2004-2011.J Viral Hepat. 2015 Nov;22(11):906-13. doi: 10.1111/jvh.12414. Epub 2015 Apr 20. J Viral Hepat. 2015. PMID: 25894392 Free PMC article.
-
Regional differences in treatment rates for patients with chronic hepatitis C infection: Systematic review and meta-analysis.PLoS One. 2017 Sep 6;12(9):e0183851. doi: 10.1371/journal.pone.0183851. eCollection 2017. PLoS One. 2017. PMID: 28877190 Free PMC article.
References
-
- National Hepatitis C Prevention Strategy. Hepatitis C Infection in the United States. Center for Disease Control. Available at: www.cdc.gov Accessed Dec 15, 2007.
-
- Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infect Dis. 2005 Sep;5(9):558–567. - PubMed
-
- Cooke GS, Main J. Improving the treatment of hepatitis C infection in the UK. Expert Opin Pharmcother. 2007 Feb;8(2):183–191. - PubMed
-
- Consensus conference. Treatment of hepatitis C. Gastroenterol Clin Biol. 2002;26 Spec No 2:B303–B320. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources