

Techniques for liver parenchymal transection in liver resection
- PMID: 19160307
- PMCID: PMC11627300
- DOI: 10.1002/14651858.CD006880.pub2
Techniques for liver parenchymal transection in liver resection
Abstract
Background: Blood loss during elective liver resection is one of the main factors affecting the surgical outcome. Different parenchymal transection techniques have been suggested to decrease blood loss.
Objectives: To assess the benefits and risks of the different techniques of parenchymal transection during liver resections.
Search strategy: We searched The Cochrane Hepato-Biliary Group Controlled Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library, MEDLINE, EMBASE, and Science Citation Index Expanded (March 2008).
Selection criteria: We considered for inclusion all randomised clinical trials comparing different methods of parenchymal dissection irrespective of the method of vascular occlusion or any other measures used for lowering blood loss.
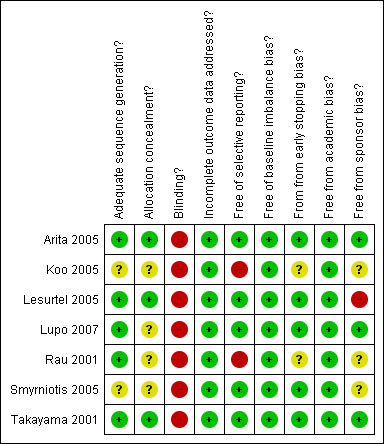
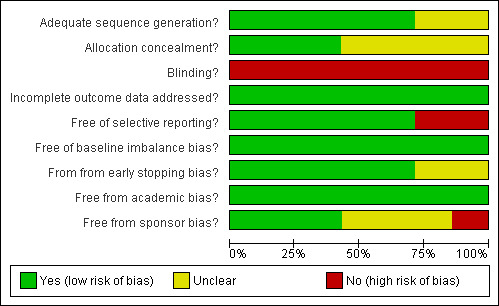
Data collection and analysis: Two authors identified the trials and extracted the data on the population characteristics, bias risk, mortality, morbidity, blood loss, transection speed, and hospital stay independently of each other. We calculated the odds ratio (OR), mean difference (MD), or standardised mean difference (SMD) with 95% confidence intervals based on 'interntion-to-treat analysis' or 'available case analysis' using RevMan 5.
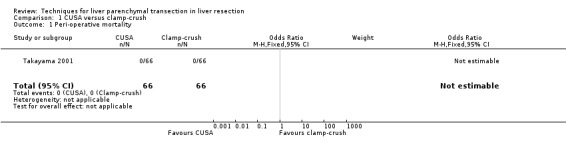
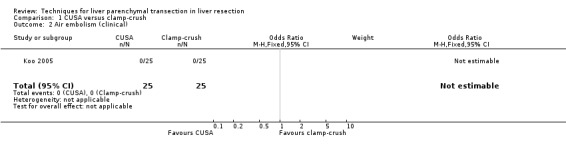
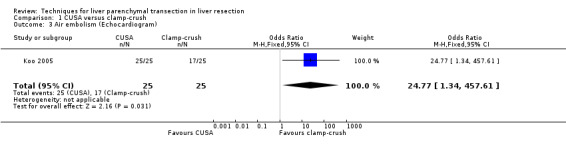
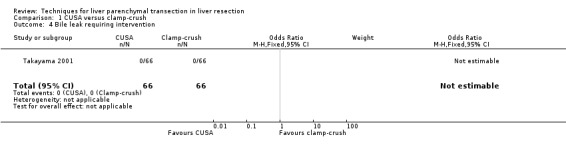
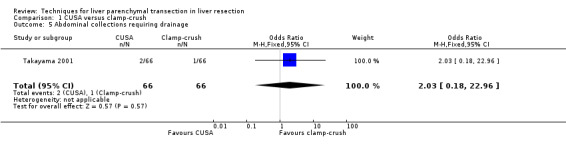
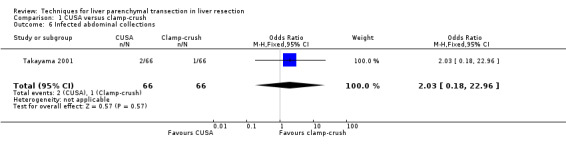
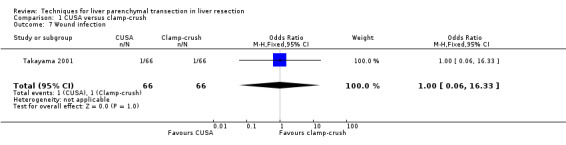
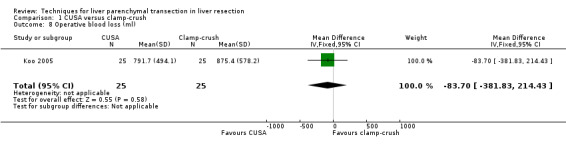
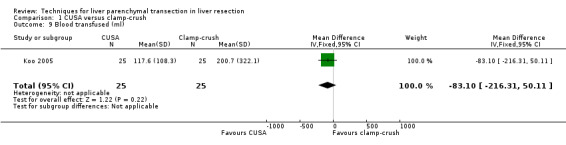
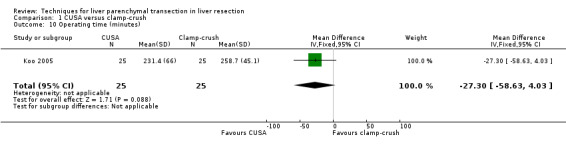
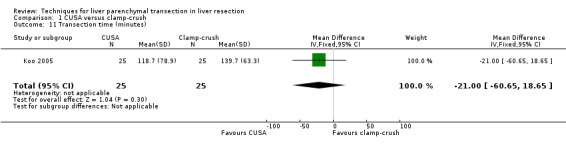
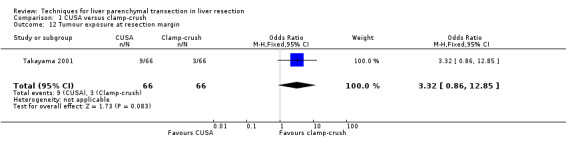
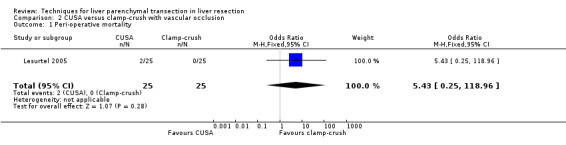
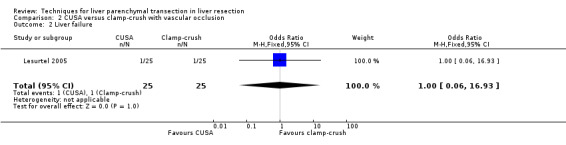
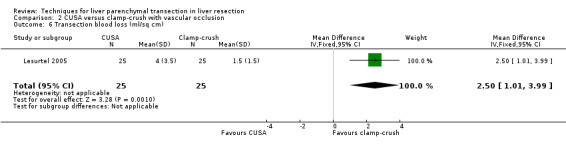
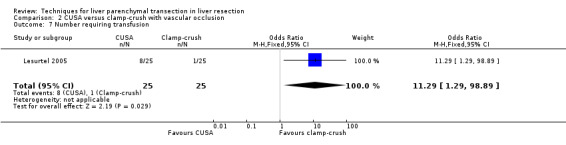
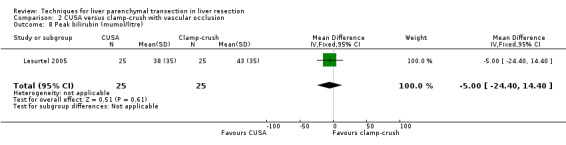
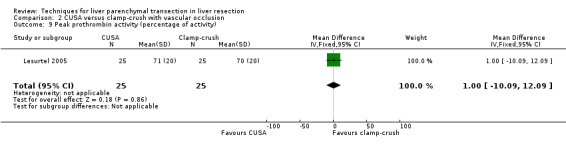
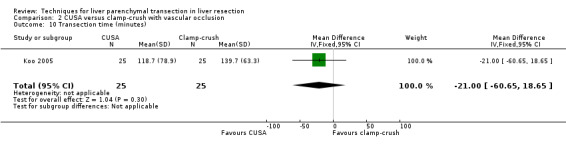
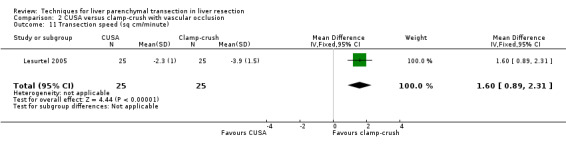
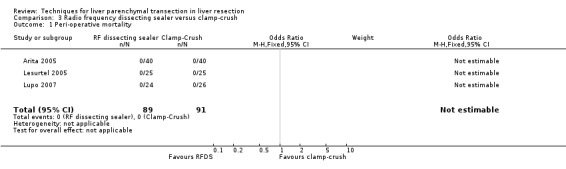
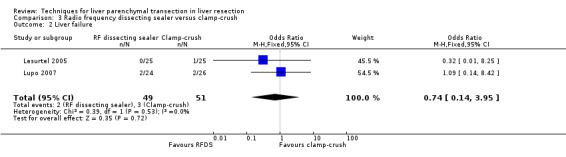
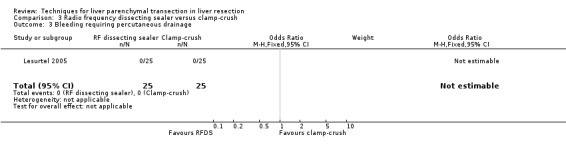
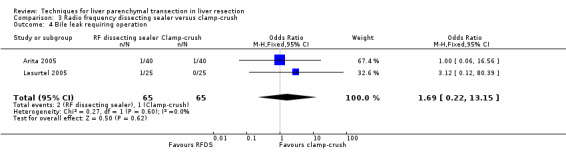
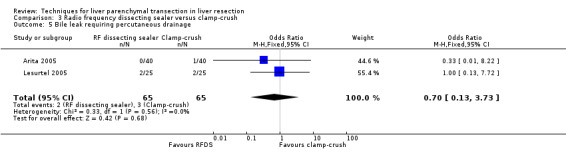
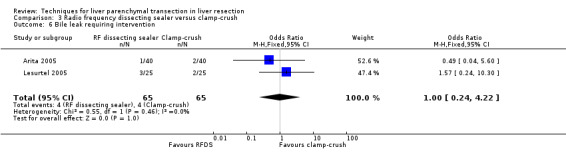
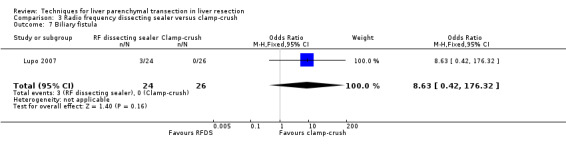
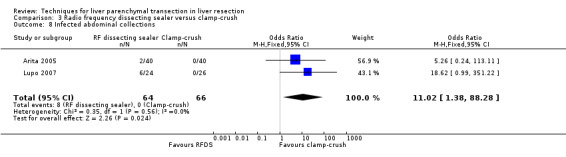
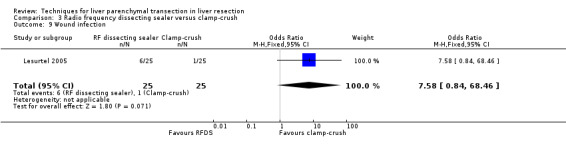
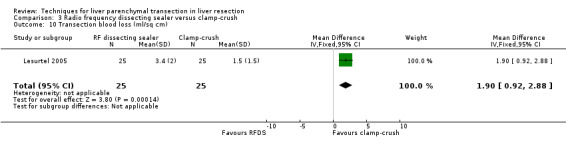
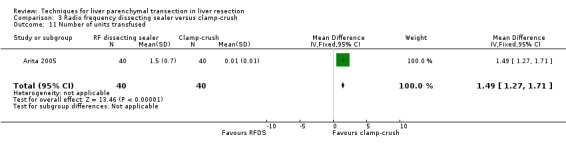
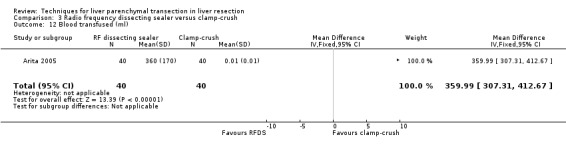
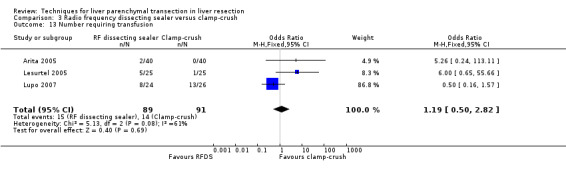
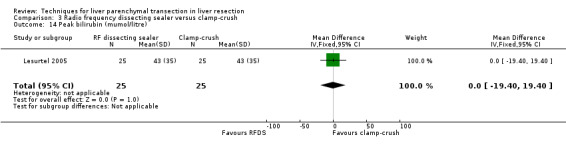
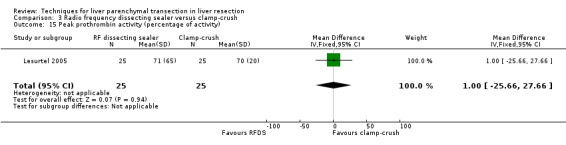
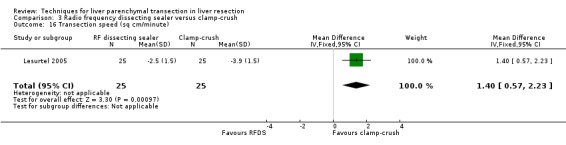
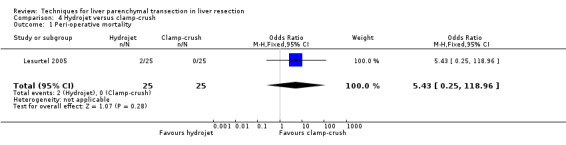
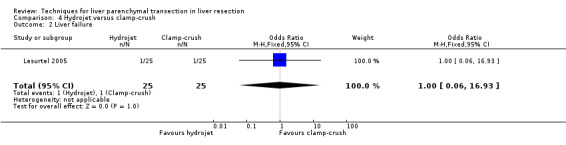
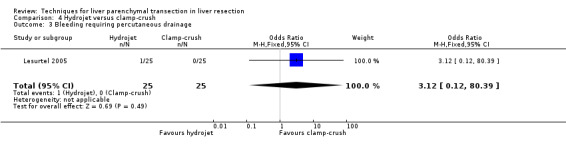
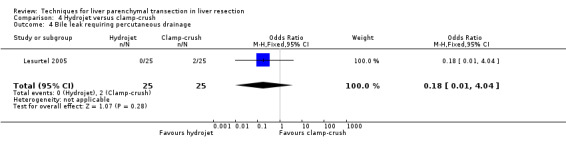
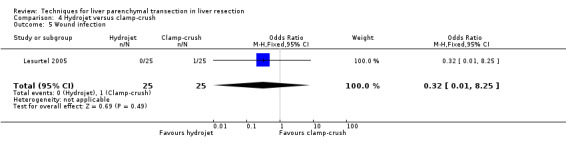
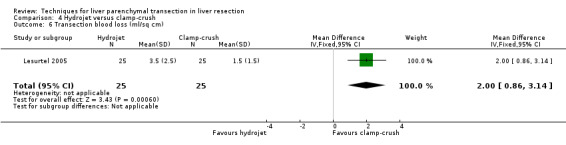
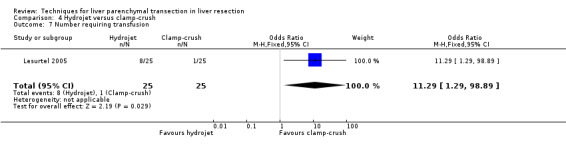
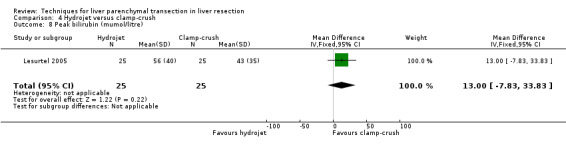
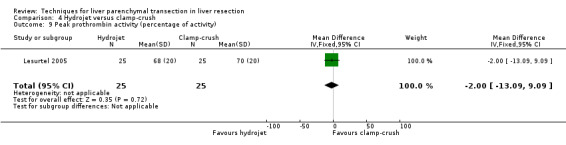
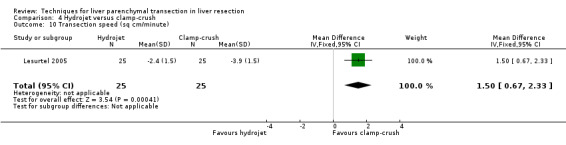
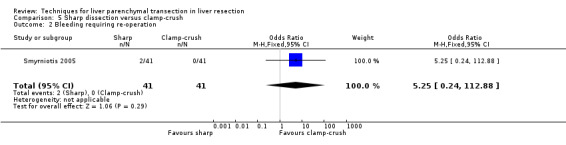
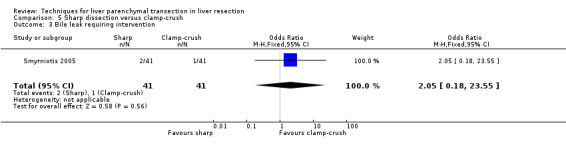
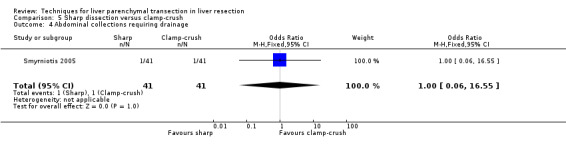
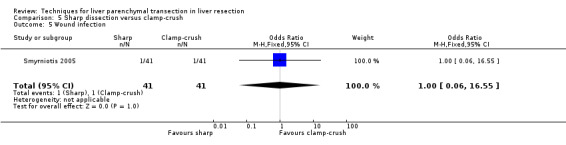
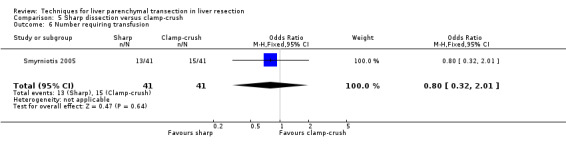
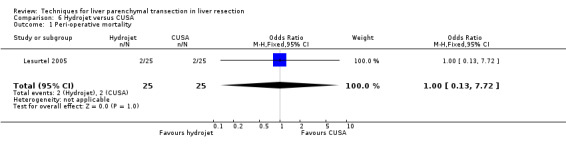
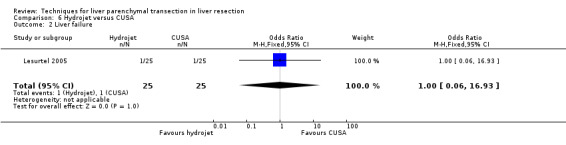
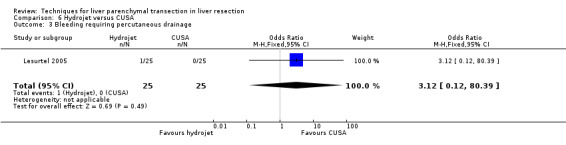
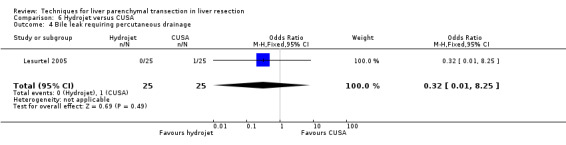
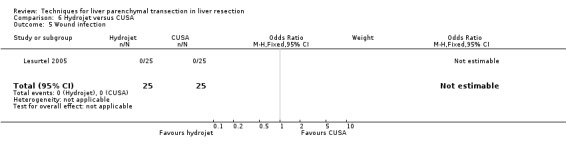
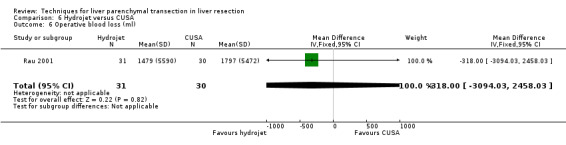
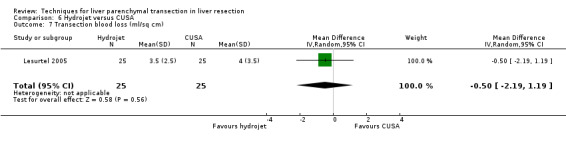
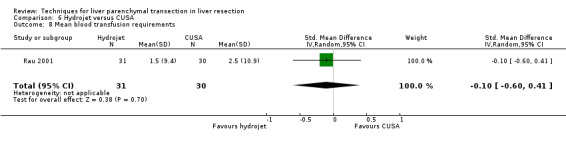
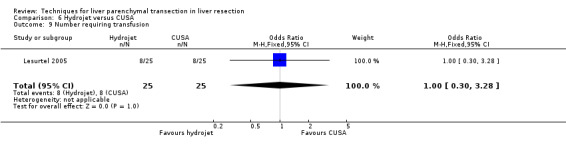
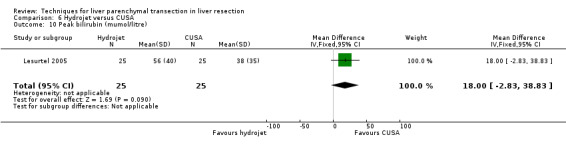
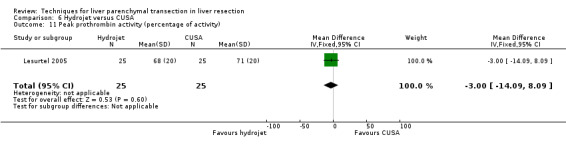
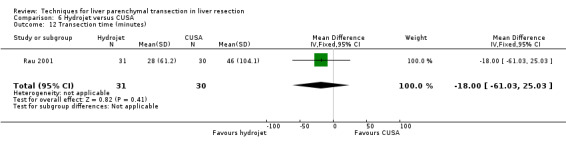
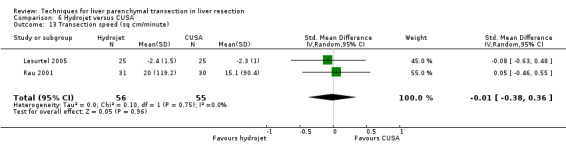
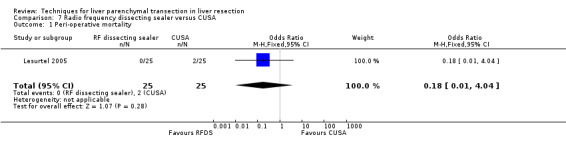
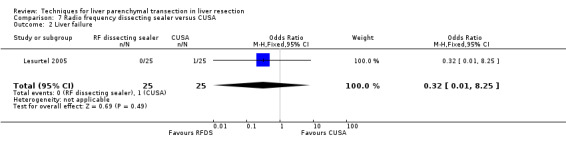
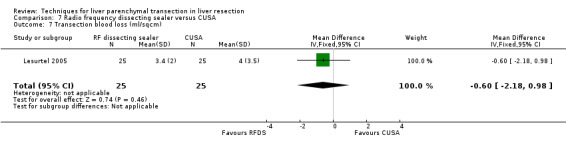
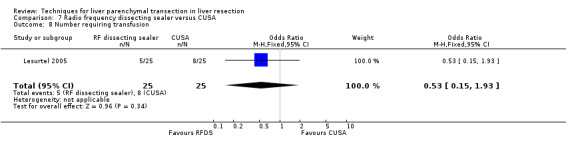
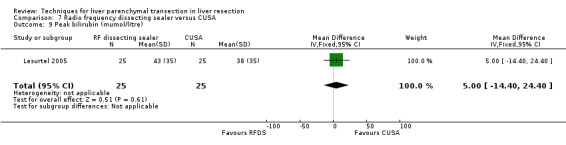
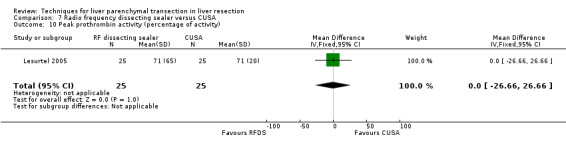
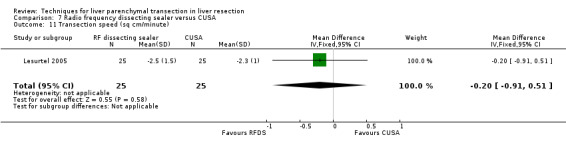
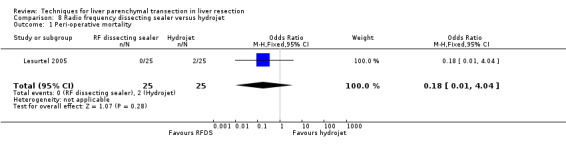
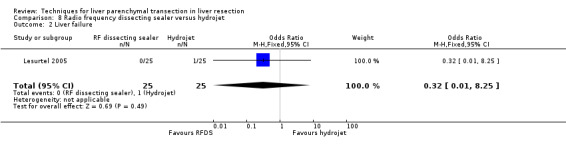
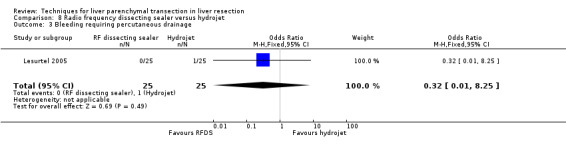
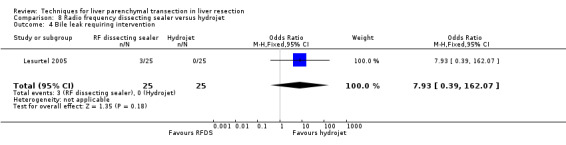
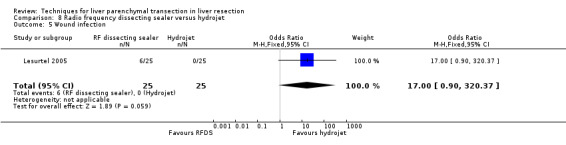
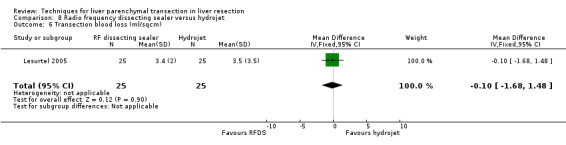
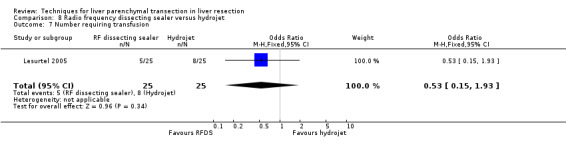
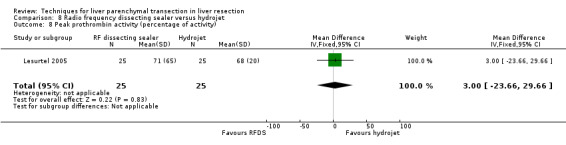
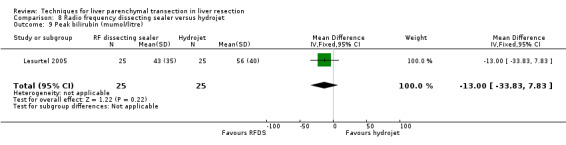
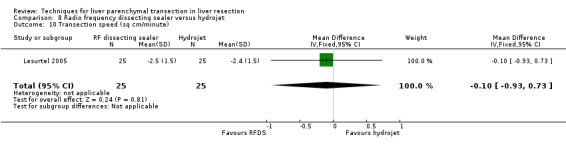
Main results: We included seven trials randomising 556 patients. The comparisons include CUSA (cavitron ultrasound surgical aspirator) versus clamp-crush (two trials); radiofrequency dissecting sealer (RFDS) versus clamp-crush (two trials); sharp dissection versus clamp-crush technique (one trial); and hydrojet versus CUSA (one trial). One trial compared CUSA, RFDS, hydrojet, and clamp-crush technique. The infective complications and transection blood loss were greater in the RFDS than clamp-crush. There was no difference in the blood transfusion requirements, intensive therapy unit (ITU) stay, or hospital stay in this comparison. There was no significant differences in the mortality, morbidity, markers of liver parenchymal injury or liver dysfunction, ITU, or hospital stay in the other comparisons. The blood transfusion requirements were lower in the clamp-crush technique than CUSA and hydrojet. There was no difference in the transfusion requirements of clamp-crush technique and sharp dissection. Clamp-crush technique is quicker than CUSA, hydrojet, and RFDS. The transection speed of sharp dissection and clamp-crush technique was not compared. There was no clinically or statistically significant difference in the operating time between sharp dissection and clamp-crush techniques. Clamp-crush technique is two to six times cheaper than the other methods depending upon the number of surgeries performed each year.
Authors' conclusions: Clamp-crush technique is advocated as the method of choice in liver parenchymal transection because it avoids special equipment, whereas the newer methods do not seem to offer any benefit in decreasing the morbidity or transfusion requirement.
Conflict of interest statement
None known.
Figures
Update of
- doi: 10.1002/14651858.CD006880
References
References to studies included in this review
Arita 2005 {published data only}
-
- Arita J, Hasegawa K, Kokudo N, Sano K, Sugawara Y, Makuuchi M. Randomized clinical trial of the effect of a saline‐linked radiofrequency coagulator on blood loss during hepatic resection. The British Journal of Surgery 2005;92(8):954‐9. - PubMed
Koo 2005 {published data only}
-
- Koo BN, Kil HK, Choi JS, Kim JY, Chun DH, Hong YW. Hepatic resection by the Cavitron Ultrasonic Surgical Aspirator increases the incidence and severity of venous air embolism. Anesthesia Analgesia 2005;101(4):966‐70, table of contents. - PubMed
Lesurtel 2005 {published and unpublished data}
Lupo 2007 {published and unpublished data}
-
- Lupo L, Gallerani A, Panzera P, Tandoi F, Palma G, Memeo V. Randomized clinical trial of radiofrequency‐assisted versus clamp‐crushing liver resection. The British Journal of Surgery 2007;94(3):287‐91. - PubMed
Rau 2001 {published and unpublished data}
-
- Rau HG, Wichmann MW, Schinkel S, Buttler E, Pickelmann S, Schauer R, et al. [Surgical techniques in hepatic resections: Ultrasonic aspirator versus Jet‐Cutter. A prospective randomized clinical trial]. Zentralblatt fur Chirurgie 2001;126(8):586‐90. - PubMed
Smyrniotis 2005 {published and unpublished data}
-
- Smyrniotis V, Arkadopoulos N, Kostopanagiotou G, Farantos C, Vassiliou J, Contis J, et al. Sharp liver transection versus clamp crushing technique in liver resections: a prospective study. Surgery 2005;137(3):306‐11. - PubMed
Takayama 2001 {published and unpublished data}
-
- Takayama T, Makuuchi M, Kubota K, Harihara Y, Hui AM, Sano K, et al. Randomized comparison of ultrasonic vs clamp transection of the liver. Archives of Surgery 2001;136(8):922‐8. - PubMed
References to studies excluded from this review
Rau 1996 {published data only}
-
- Rau HG, Meyer G, Jauch KW, Cohnert TU, Buttler E, Schildberg FW. [Liver resection with the water jet: conventional and laparoscopic surgery]. Der Chirurg 1996;67(5):546‐51. - PubMed
Additional references
Belghiti 1993
Belghiti 1996
Belghiti 1999
Bombuy 2004
-
- Bombuy E, Fondevila C, Rodriguez‐Laiz G, Ferrer J, Amador A, Valentini M, et al. Ischemic preconditioning in adult living donor liver transplantation, a pilot study [EASL abstract]. Journal of Hepatology 2004;40(Suppl 1):39.
DeMets 1987
-
- DeMets DL. Methods for combining randomized clinical trials: strengths and limitations. Statistics in Medicine 1987;6(3):341‐50. - PubMed
DerSimonian 1986
-
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. - PubMed
Egger 1997
Fong 1996
-
- Fong Y, Brennan MF, Brown K, Heffernan N, Blumgart LH. Drainage is unnecessary after elective liver resection. American Journal of Surgery 1996;171(1):158‐62. - PubMed
Gluud 2008
-
- Gluud C, Nikolova D, Klingenberg SL, Whitfield K, Alexakis N, Als‐Nielsen B, et al. Cochrane Hepato‐Biliary Group. About The Cochrane Collaboration (Cochrane Review Groups (CRGs)) 2008, Issue 4. Art. No.: LIVER.
Gurusamy 2007
-
- Gurusamy KS, Kumar Y, Sharma D, Davidson BR. Methods of vascular occlusion for elective liver resections. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD006409.pub2] - PubMed
Hasegawa 2002
-
- Hasegawa K, Takayama T, Orii R, Sano K, Sugawara Y, Imamura H, et al. Effect of hypoventilation on bleeding during hepatic resection: a randomized controlled trial. Archives of Surgery 2002;137(3):311‐5. - PubMed
HES 2005
-
- Hospital Episode Statistics. Main operations. 3 character: 2004‐05. http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&c... (accessed 9 September 2008).
Higgins 2002
-
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. - PubMed
Higgins 2008
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Intervention 5.0.0 [updated February 2008]. The Cochrane Colloboration, 2008. Available from www.cochrane‐handbook.org.
Ibrahim 2006
-
- Ibrahim S, Chen CL, Lin CC, Yang CH, Wang CC, Wang SH, et al. Intraoperative blood loss is a risk factor for complications in donors after living donor hepatectomy. Liver Transplantation 2006;12(6):950‐7. - PubMed
Kjaergard 2001
-
- Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and discrepancies between large and small randomized trials in meta‐analyses. Annals of Internal Medicine 2001;135(11):982‐9. - PubMed
Lin 1987
-
- Lin TY, Lee CS, Chen KM, Chen CC. Role of surgery in the treatment of primary carcinoma of the liver: a 31‐year experience. The British Journal of Surgery 1987;74(9):839‐42. [PUBMED: 2822201] - PubMed
Liu 2004
Macaskill 2001
-
- Macaskill P, Walter SD, Irwig L. A comparison of methods to detect publication bias in meta‐analysis. Statistics in Medicine 2001;20(4):641‐54. - PubMed
Moher 1998
-
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352(9128):609‐13. - PubMed
Newell 1992
-
- Newell DJ. Intention‐to‐treat analysis: implications for quantitative and qualitative research. International Journal of Epidemiology 1992;21(5):837‐41. - PubMed
RevMan 2008 [Computer program]
-
- Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008.
Royle 2003
-
- Royle P, Milne R. Literature searching for randomized controlled trials used in Cochrane reviews: rapid versus exhaustive searches. International Journal of Technology Assessment in Health Care 2003;19(4):591‐603. - PubMed
Rui 2003
Schulz 1995
-
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273(5):408‐12. - PubMed
Shimada 1998
-
- Shimada M, Takenaka K, Fujiwara Y, Gion T, Shirabe K, Yanaga K, et al. Risk factors linked to postoperative morbidity in patients with hepatocellular carcinoma. British Journal of Surgery 1998;85(2):195‐8. - PubMed
Smyrniotis 2002
-
- Smyrniotis VE, Kostopanagiotou GG, Gamaletsos EL, Vassiliou JG, Voros DC, Fotopoulos AC, et al. Total versus selective hepatic vascular exclusion in major liver resections. American Journal of Surgery 2002;183(2):173‐8. - PubMed
Strasberg 2000
-
- Strasberg SM, Belghiti J, Clavien PA, Gadzijev E, Garden JO, Lau WY, et al. The Brisbane 2000 terminology of liver anatomy and resections. HPB Surgery 2000;2(3):333‐9.
Sweeting 2004
-
- Sweeting MJ, Sutton AJ, Lambert PC. What to add to nothing? Use and avoidance of continuity corrections in meta‐analysis of sparse data. Statistics in Medicine 2004;23(9):1351‐75. - PubMed
Wang 2006
Weber 2002
Wood 2008
Yoshimura 2004
-
- Yoshimura Y, Kubo S, Shirata K, Hirohashi K, Tanaka H, Shuto T, et al. Risk factors for postoperative delirium after liver resection for hepatocellular carcinoma. World Journal of Surgery 2004;28(10):982‐6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical