

Comparison of mannitol and methacholine to predict exercise-induced bronchoconstriction and a clinical diagnosis of asthma
- PMID: 19161635
- PMCID: PMC2644668
- DOI: 10.1186/1465-9921-10-4
Comparison of mannitol and methacholine to predict exercise-induced bronchoconstriction and a clinical diagnosis of asthma
Abstract
Background: Asthma can be difficult to diagnose, but bronchial provocation with methacholine, exercise or mannitol is helpful when used to identify bronchial hyperresponsiveness (BHR), a key feature of the disease. The utility of these tests in subjects with signs and symptoms of asthma but without a clear diagnosis has not been investigated. We investigated the sensitivity and specificity of mannitol to identify exercise-induced bronchoconstriction (EIB) as a manifestation of BHR; compared this with methacholine; and compared the sensitivity and specificity of mannitol and methacholine for a clinician diagnosis of asthma.
Methods: 509 people (6-50 yr) were enrolled, 78% were atopic, median FEV1 92.5% predicted, and a low NAEPPII asthma score of 1.2. Subjects with symptoms of seasonal allergy were excluded. BHR to exercise was defined as a > or = 10% fall in FEV1 on at least one of two tests, to methacholine a PC20 < or = 16 mg/ml and to mannitol a 15% fall in FEV1 at < or = 635 mg or a 10% fall between doses. The clinician diagnosis of asthma was made on examination, history, skin tests, questionnaire and response to exercise but they were blind to the mannitol and methacholine results.
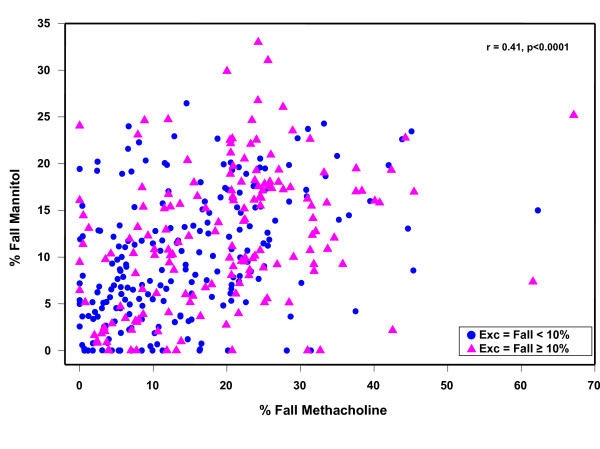
Results: Mannitol and methacholine were therapeutically equivalent to identify EIB, a clinician diagnosis of asthma, and prevalence of BHR. The sensitivity/specificity of mannitol to identify EIB was 59%/65% and for methacholine it was 56%/69%. The BHR was mild. Mean EIB % fall in FEV1 in subjects positive to exercise was 19%, (SD 9.2), mannitol PD15 158 (CI:129,193) mg, and methacholine PC20 2.1(CI:1.7, 2.6) mg/ml. The prevalence of BHR was the same: for exercise (43.5%), mannitol (44.8%), and methacholine (41.6%) with a test agreement between 62 & 69%. The sensitivity and specificity for a clinician diagnosis of asthma was 56%/73% for mannitol and 51%/75% for methacholine. The sensitivity increased to 73% and 72% for mannitol and methacholine when two exercise tests were positive.
Conclusion: In this group with normal FEV1, mild symptoms, and mild BHR, the sensitivity and specificity for both mannitol and methacholine to identify EIB and a clinician diagnosis of asthma were equivalent, but lower than previously documented in well-defined populations.
Trial registration: This was a multi-center trial comprising 25 sites across the United States of America.
Trial registration: ClinicalTrials.gov NCT00025229.
Figures


References
-
- Expert Panel Report Update on Selected Topics 2002: National Asthma Education and Prevention Program. National Institutes of Health, National Heart, Lung and Blood Institute, 2003. NIH publication no. 02-5074. 2003.
-
- Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, MacIntyre NR, McKay RT, Wanger JS, Anderson SD, Cockcroft DW, Fish JE, Sterk PJ. Guidelines for methacholine and exercise challenge testing – 1999. Am J Respir Crit Care Med. 2000;161:309–329. - PubMed
-
- Sterk PJ, Fabbri LM, Quanjer PH, Cockcroft DW, O'Byrne PM, Anderson SD, Juniper EF, Malo J-L. Airway responsiveness: Standardized challenge testing with pharmacological, physical and sensitizing stimuli in adults. Eur Respir J Suppl. 1993;16:53–83. - PubMed
-
- Cockcroft DW. How best to measure airway responsiveness. Am J Respir Crit Care Med. 2001;163:1514–1515. - PubMed
