

Complete pathologic response after neoadjuvant chemoradiotherapy for esophageal cancer is associated with enhanced survival
- PMID: 19161745
- PMCID: PMC2930775
- DOI: 10.1016/j.athoracsur.2008.11.001
Complete pathologic response after neoadjuvant chemoradiotherapy for esophageal cancer is associated with enhanced survival
Abstract
Background: Neoadjuvant chemoradiotherapy followed by esophagogastrectomy has become the standard of care for patients with locally advanced esophageal cancer. This report analyzes our experience with this treatment approach.
Methods: From January 1998 through December 2003, all patients from a single institution receiving neoadjuvant chemoradiotherapy followed by esophagogastrectomy were reviewed for operative mortality, morbidity, long-term survival, and factors affecting survival. Only patients preoperatively staged with both computed tomographic scans and endoscopic ultrasound were included.
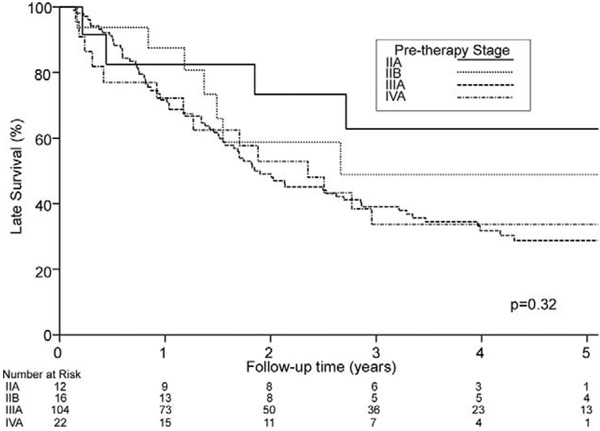
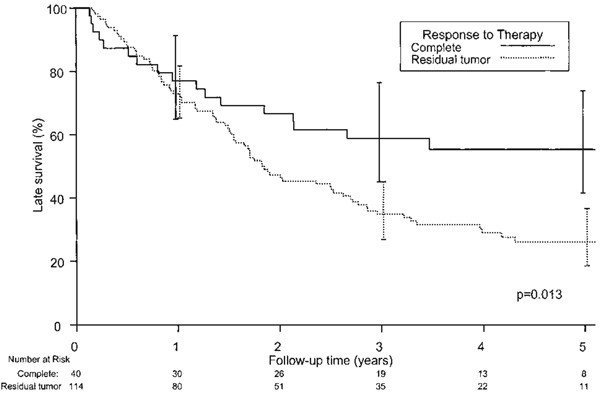
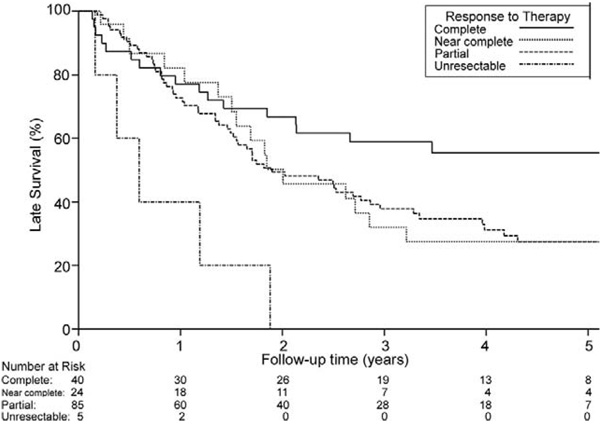
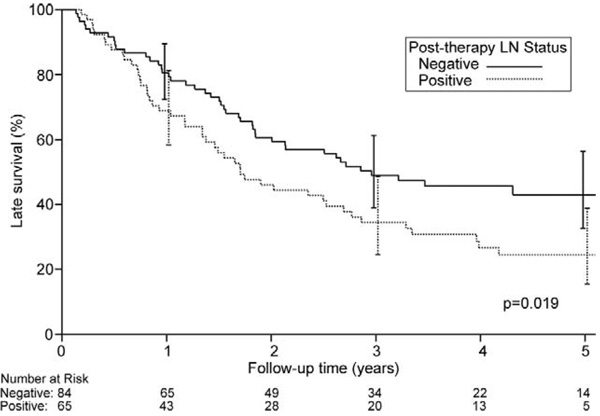
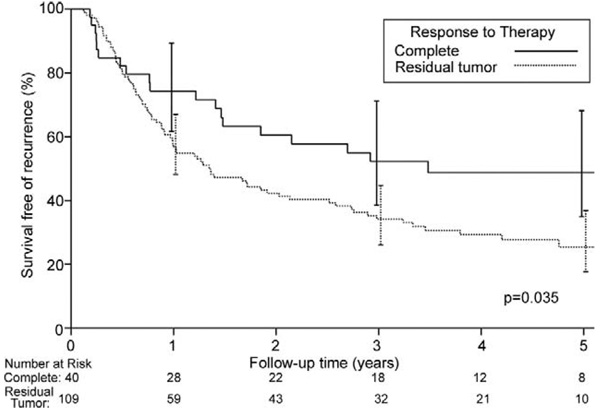
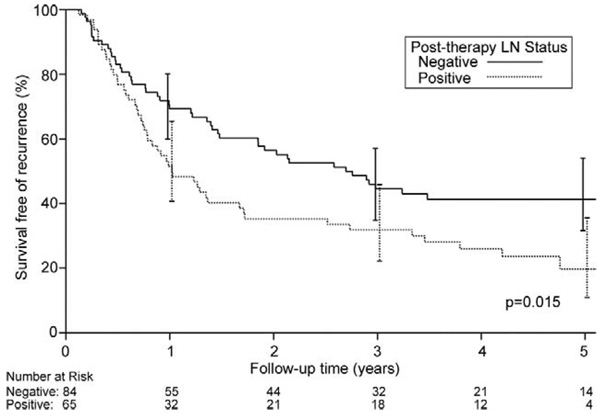
Results: There were 162 patients (142 men, 20 women), and the median age was 61 years (range, 22 to 81 years). Histopathology was adenocarcinoma in 143 patients and squamous cell in 19. Pretreatment clinical stage was II in 28 patients (17%), III in 111 (68%), and IV (M1a) in 23 (14%). Ivor Lewis esophagogastrectomy was the most common procedure, occurring in 132 patients. Operative mortality and morbidity was 4.9% and 37%, respectively. Pathologic response was complete in 42 patients (26%), near complete in 27 (17%), partial in 88 (54%), and unresectable in 5 (3%). Five-year survival for overall, complete, near complete, and partial response patients was 34%, 55%, 27%, and 27%, respectively (p = 0.013). Patients whose lymph nodes were rendered free of cancer showed improved overall and disease-free survival compared with patients having persistently positive lymph nodes (p = 0.019).
Conclusions: Esophagogastrectomy after neoadjuvant chemoradiotherapy can be performed with low mortality and morbidity. Patients with complete pathologic response have significantly improved long-term survival compared with patients with near complete and partial responses. Future efforts should be directed at understanding determinants of complete responses.
Figures
Similar articles
-
Sex Disparities After Induction Chemoradiotherapy and Esophagogastrectomy for Esophageal Cancer.Ann Thorac Surg. 2017 Oct;104(4):1147-1152. doi: 10.1016/j.athoracsur.2017.05.030. Epub 2017 Aug 22. Ann Thorac Surg. 2017. PMID: 28842111
-
Outcomes With Open and Minimally Invasive Ivor Lewis Esophagectomy After Neoadjuvant Therapy.Ann Thorac Surg. 2016 Mar;101(3):1097-103. doi: 10.1016/j.athoracsur.2015.09.062. Epub 2015 Dec 1. Ann Thorac Surg. 2016. PMID: 26652140
-
Long-term survival based on pathologic response to neoadjuvant therapy in esophageal cancer.J Surg Res. 2017 Aug;216:65-72. doi: 10.1016/j.jss.2017.03.022. Epub 2017 Mar 31. J Surg Res. 2017. PMID: 28807215
-
Utility of PET, CT, and EUS to identify pathologic responders in esophageal cancer.Ann Thorac Surg. 2004 Oct;78(4):1152-60; discussion 1152-60. doi: 10.1016/j.athoracsur.2004.04.046. Ann Thorac Surg. 2004. PMID: 15464463 Review.
-
Neoadjuvant chemotherapy or chemoradiotherapy for locally advanced esophageal cancer.Thorac Surg Clin. 2013 Nov;23(4):509-23. doi: 10.1016/j.thorsurg.2013.07.005. Epub 2013 Oct 13. Thorac Surg Clin. 2013. PMID: 24199701 Review.
Cited by
-
Prognostic relevance of lymph node regression on survival in esophageal cancer: a systematic review and meta-analysis.Dis Esophagus. 2022 Jan 7;35(1):doab021. doi: 10.1093/dote/doab021. Dis Esophagus. 2022. PMID: 33893494 Free PMC article.
-
Clinical parameters model for predicting pathologic complete response following preoperative chemoradiation in patients with esophageal cancer.Ann Oncol. 2012 Oct;23(10):2638-2642. doi: 10.1093/annonc/mds210. Epub 2012 Jul 24. Ann Oncol. 2012. PMID: 22831985 Free PMC article.
-
A Survival Prediction Nomogram for Esophageal Squamous Cell Carcinoma Treated with Neoadjuvant Chemoradiotherapy Followed by Surgery.Cancer Manag Res. 2021 Oct 9;13:7771-7782. doi: 10.2147/CMAR.S329687. eCollection 2021. Cancer Manag Res. 2021. PMID: 34675672 Free PMC article.
-
Perioperative chemotherapy for gastroesophageal cancer in British Columbia: a multicentre experience.Curr Oncol. 2014 Apr;21(2):77-83. doi: 10.3747/co.21.1788. Curr Oncol. 2014. PMID: 24764696 Free PMC article.
-
A preoperative predictive model based on multi-modal features to predict pathological complete response after neoadjuvant chemoimmunotherapy in esophageal cancer patients.Front Immunol. 2025 Jan 27;16:1530279. doi: 10.3389/fimmu.2025.1530279. eCollection 2025. Front Immunol. 2025. PMID: 39958355 Free PMC article.
References
-
- Cancer Facts & Figures 2007. American Cancer Society, Inc; 2007.
-
- Visbal AL, Allen MS, Miller DL, Deschamps C, Trastek VF, Pairolero PC. Ivor Lewis esophagogastrectomy for esophageal cancer. Ann Thorac Surg. 2001;71:1803–1808. - PubMed
-
- Jaroszewski DE, Deschamps C, Gunderson LL, Lanza LA, Trastek VF, Pairolero PC. Cancer of the esophagus. In: Kelly KA, Sarr MG, Hinder RA, editors. Mayo Clinic gastrointestinal surgery. Philadelphia, PA: WB Saunders; 2004. pp. 57–73.
-
- Chak B, Forastiere AA. Neoadjuvant therapy for esophageal cancer. In: Yang CY, Cameron DE, editors. Current therapy in thoracic and cardiovascular surgery. Philadelphia, PA: Mosby; 2004. pp. 356–360.
-
- Behzadi A, Nichols FC, Cassivi SD, Deschamps C, Allen MS, Pairolero PC. Esophagogastrectomy: the influence of stapled versus hand-sewn anastomosis on outcome. J Gastrointest Surg. 2005;9:1031–1040. - PubMed
