

Coronary calcium predicts events better with absolute calcium scores than age-sex-race/ethnicity percentiles: MESA (Multi-Ethnic Study of Atherosclerosis)
- PMID: 19161884
- PMCID: PMC2652569
- DOI: 10.1016/j.jacc.2008.07.072
Coronary calcium predicts events better with absolute calcium scores than age-sex-race/ethnicity percentiles: MESA (Multi-Ethnic Study of Atherosclerosis)
Erratum in
- J Am Coll Cardiol. 2009 Apr 21;53(16):1474
Abstract
Objectives: In this study, we aimed to establish whether age-sex-specific percentiles of coronary artery calcium (CAC) predict cardiovascular outcomes better than the actual (absolute) CAC score.
Background: The presence and extent of CAC correlates with the overall magnitude of coronary atherosclerotic plaque burden and with the development of subsequent coronary events.
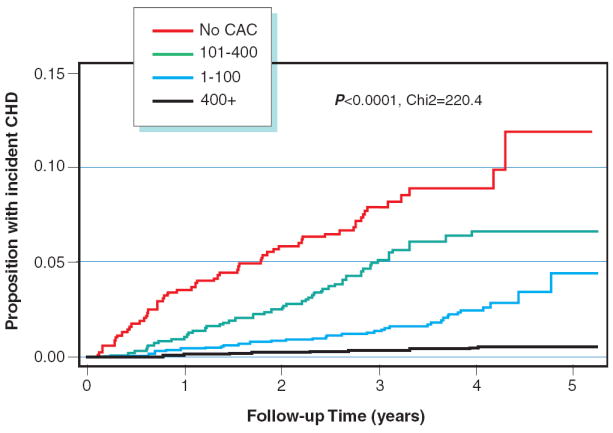
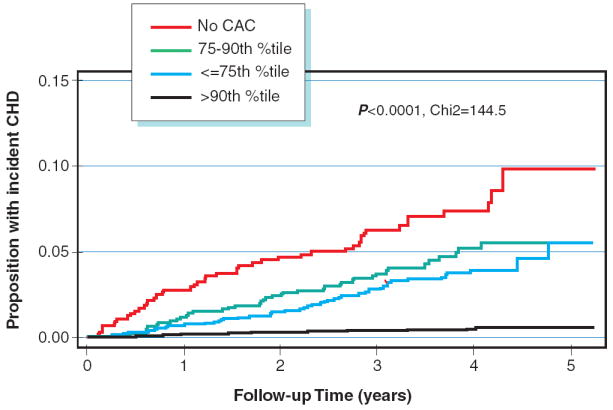
Methods: MESA (Multi-Ethnic Study of Atherosclerosis) is a prospective cohort study of 6,814 asymptomatic participants followed for coronary heart disease (CHD) events including myocardial infarction, angina, resuscitated cardiac arrest, or CHD death. Time to incident CHD was modeled with Cox regression, and we compared models with percentiles based on age, sex, and/or race/ethnicity to categories commonly used (0, 1 to 100, 101 to 400, 400+ Agatston units).
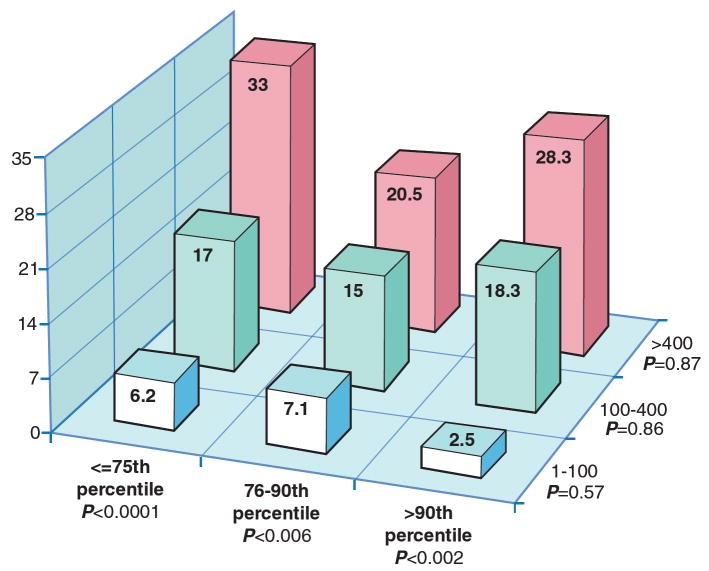
Results: There were 163 (2.4%) incident CHD events (median follow-up 3.75 years). Expressing CAC in terms of age- and sex-specific percentiles had significantly lower area under the receiver-operating characteristic curve (AUC) than when using absolute scores (women: AUC 0.73 versus 0.76, p = 0.044; men: AUC 0.73 versus 0.77, p < 0.001). Akaike's information criterion indicated better model fit with the overall score. Both methods robustly predicted events (>90th percentile associated with a hazard ratio [HR] of 16.4, 95% confidence interval [CI]: 9.30 to 28.9, and score >400 associated with HR of 20.6, 95% CI: 11.8 to 36.0). Within groups based on age-, sex-, and race/ethnicity-specific percentiles there remains a clear trend of increasing risk across levels of the absolute CAC groups. In contrast, once absolute CAC category is fixed, there is no increasing trend across levels of age-, sex-, and race/ethnicity-specific categories. Patients with low absolute scores are low-risk, regardless of age-, sex-, and race/ethnicity-specific percentile rank. Persons with an absolute CAC score of >400 are high risk, regardless of percentile rank.
Conclusions: Using absolute CAC in standard groups performed better than age-, sex-, and race/ethnicity-specific percentiles in terms of model fit and discrimination. We recommend using cut points based on the absolute CAC amount, and the common CAC cut points of 100 and 400 seem to perform well.
Figures
Comment in
-
Are you as old as your arteries or as old as your coronary artery calcification score?J Am Coll Cardiol. 2009 Jan 27;53(4):353-4. doi: 10.1016/j.jacc.2008.08.075. J Am Coll Cardiol. 2009. PMID: 19161885 No abstract available.
-
Don't throw the baby out with the bath water.J Am Coll Cardiol. 2009 Aug 4;54(6):574; author reply 574-5. doi: 10.1016/j.jacc.2009.02.083. J Am Coll Cardiol. 2009. PMID: 19643326 No abstract available.
References
-
- Arad Y, Roth M, Newstein D, et al. Coronary calcification, coronary risk factors, and atherosclerotic cardiovascular disease events. The St. Francis Heart Study. J Am Coll Cardiol. 2005;46:158–165. - PubMed
-
- Taylor AJ, Bindeman J, Feuerstein I, Cao F, Brazaitis M, O’Malley PG. Coronary Calcium Independently Predicts Incident Premature Coronary Heart Disease Over Measured Cardiovascular Risk Factors. J Am Coll Cardiol. 2005;46:807–14. - PubMed
-
- Vliegenthart R, Oudkerk M, Hofman A, Oei HH, van Dijck W, van Rooij FJ, Witteman JC. Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation. 2005 Jul 26;112(4):572–7. - PubMed
-
- Budoff MJ, Shaw LJ, Liu ST, Weinstein SR, Mosler TP, Tseng PH, Flores FR, Callister TQ, Raggi P, Berman DS. Long-Term Prognosis Associated With Coronary Calcification: Observations From a Registry of 25,253 Patients. J Am Coll Cardiol. 2007;49:1860–1870. - PubMed
-
- Budoff MJ, Achenbach S, Blumenthal RS, Carr JJ, Goldin JG, Greenland P, Guerci AD, Lima JAC, Rader DJ, Rubin GD, Shaw LJ, Wiegers SE. Assessment of Coronary Artery Disease by Cardiac Computed Tomography, A Scientific Statement From the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation. 2006;114(16):1761–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
