

Long-term control of disseminated pleomorphic xanthoastrocytoma with anaplastic features by means of stereotactic irradiation
- PMID: 19164434
- PMCID: PMC2743225
- DOI: 10.1215/15228517-2008-112
Long-term control of disseminated pleomorphic xanthoastrocytoma with anaplastic features by means of stereotactic irradiation
Abstract
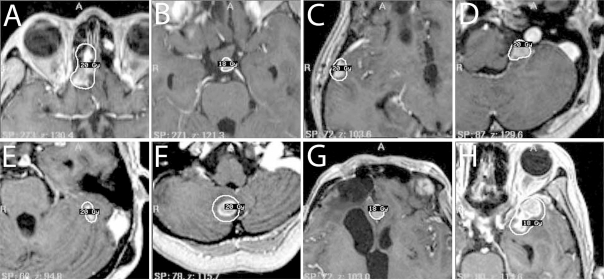
Pleomorphic xanthoastrocytoma (PXA) is a rare astrocytic neoplasm of the brain. Some PXAs are accompanied by anaplastic features and are difficult to manage because of frequent recurrences that lead to early death. No previous reports have demonstrated consistent efficacy of adjuvant radiotherapy or chemotherapy for this disease. We report a case of PXA with anaplastic features treated with stereotactic irradiation (STI) that resulted in long-term control of repeatedly recurring nodules throughout the neuraxis. A 47-year-old woman presented with an epileptic seizure due to a large tumor in the right frontal lobe. The tumor was resected and diagnosed as PXA with anaplastic features. Sixteen months later, a relapse at the primary site was noted and treated with stereotactic radiosurgery using Gamma Knife. Two years later, the patient developed a tumor nodule in the cervical spinal cord that histologically corresponded to a small-cell glioma with high cellularity and prominent MIB-1 (mindbomb homolog 1) labeling. In the following months, multiple nodular lesions appeared throughout the CNS, and STI was performed six times for eight intracranial lesions using Gamma Knife and twice using a linear accelerator, for three spinal cord lesions in total. All lesions treated with STI were well controlled, and the patient was free from symptomatic progression for 50 months. However, diffuse dissemination along the craniospinal axis eventually progressed, and she died 66 months after initial diagnosis. Autopsy showed that the nodules remained well demarcated from the surrounding nervous system tissue. STI may be an effective therapeutic tool for controlling nodular dissemination of PXA with anaplastic features.
Figures




References
-
- Giannini C, Scheithauer BW, Burger PC, et al. Pleomorphic xanthoastrocytoma: what do we really know about it? Cancer. 1999;85:2033–2045. - PubMed
-
- Gomez JG, Garcia JH, Colon LE. A variant of cerebral glioma called pleomorphic xanthoastrocytoma: case report. Neurosurgery. 1985;16:703–706. - PubMed
-
- Kepes JJ, Rubinstein LJ, Eng LF. Pleomorphic xanthoastrocytoma: a distinctive meningocerebral glioma of young subjects with relatively favorable prognosis. A study of 12 cases. Cancer. 1979;44:1839–1852. - PubMed
-
- Cervoni L, Salvati M, Santoro A, Celli P. Pleomorphic xanthoastrocytoma: some observations. Neurosurg Rev. 1996;19:13–16. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
