

Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension
- PMID: 19164700
- PMCID: PMC2720125
- DOI: 10.1164/rccm.200811-1691OC
Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension
Abstract
Rationale: Transthoracic Doppler echocardiography is recommended for screening for the presence of pulmonary hypertension (PH). However, some recent studies have suggested that Doppler echocardiographic pulmonary artery pressure estimates may frequently be inaccurate.
Objectives: Evaluate the accuracy of Doppler echocardiography for estimating pulmonary artery pressure and cardiac output.
Methods: We conducted a prospective study on patients with various forms of PH who underwent comprehensive Doppler echocardiography within 1 hour of a clinically indicated right-heart catheterization to compare noninvasive hemodynamic estimates with invasively measured values.
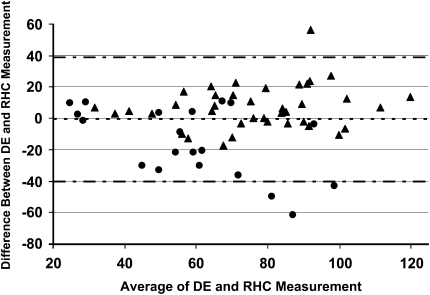
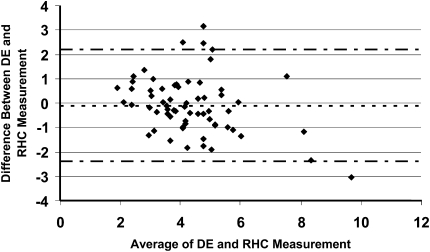
Measurements and main results: A total of 65 patients completed the study protocol. Using Bland-Altman analytic methods, the bias for the echocardiographic estimates of the pulmonary artery systolic pressure was -0.6 mm Hg with 95% limits of agreement ranging from +38.8 to -40.0 mm Hg. Doppler echocardiography was inaccurate (defined as being greater than +/-10 mm Hg of the invasive measurement) in 48% of cases. Overestimation and underestimation of pulmonary artery systolic pressure by Doppler echocardiography occurred with a similar frequency (16 vs. 15 instances, respectively). The magnitude of pressure underestimation was greater than overestimation (-30 +/- 16 vs. +19 +/- 11 mm Hg; P = 0.03); underestimates by Doppler also led more often to misclassification of the severity of the PH. For cardiac output measurement, the bias was -0.1 L/min with 95% limits of agreement ranging from +2.2 to -2.4 L/min.
Conclusions: Doppler echocardiography may frequently be inaccurate in estimating pulmonary artery pressure and cardiac output in patients being evaluated for PH.
Figures

References
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343–349. - PubMed
-
- Barst RJ, McGoon M, Torbicki A, Sitbon O, Krowka MJ, Olschewski H, Gaine S. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:40S–47S. - PubMed
-
- Forfia PR, Fisher MR, Mathai SC, Housten-Harris T, Hemnes AR, Borlaug BA, Chamera E, Corretti MC, Champion HC, Abraham TP, et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med 2006;174:1034–1041. - PubMed
-
- Hinderliter AL, Willis PW, Long W, Clarke WR, Ralph D, Caldwell EJ, Williams W, Ettinger NA, Hill NS, Summer WR, et al. Frequency and prognostic significance of pericardial effusion in primary pulmonary hypertension. PPH Study Group. Primary pulmonary hypertension. Am J Cardiol 1999;84:481–484. - PubMed
-
- Raymond RJ, Hinderliter AL, Willis PW, Ralph D, Caldwell EJ, Williams W, Ettinger NA, Hill NS, Summer WR, de Boisblanc B, et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol 2002;39:1214–1219. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
