

Postreceptor insulin resistance contributes to human dyslipidemia and hepatic steatosis
- PMID: 19164855
- PMCID: PMC2631303
- DOI: 10.1172/JCI37432
Postreceptor insulin resistance contributes to human dyslipidemia and hepatic steatosis
Abstract
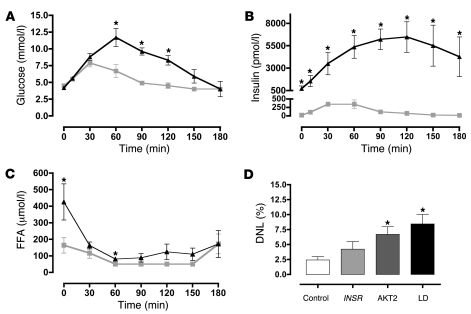
Metabolic dyslipidemia is characterized by high circulating triglyceride (TG) and low HDL cholesterol levels and is frequently accompanied by hepatic steatosis. Increased hepatic lipogenesis contributes to both of these problems. Because insulin fails to suppress gluconeogenesis but continues to stimulate lipogenesis in both obese and lipodystrophic insulin-resistant mice, it has been proposed that a selective postreceptor defect in hepatic insulin action is central to the pathogenesis of fatty liver and hypertriglyceridemia in these mice. Here we show that humans with generalized insulin resistance caused by either mutations in the insulin receptor gene or inhibitory antibodies specific for the insulin receptor uniformly exhibited low serum TG and normal HDL cholesterol levels. This was due at least in part to surprisingly low rates of de novo lipogenesis and was associated with low liver fat content and the production of TG-depleted VLDL cholesterol particles. In contrast, humans with a selective postreceptor defect in AKT2 manifest increased lipogenesis, elevated liver fat content, TG-enriched VLDL, hypertriglyceridemia, and low HDL cholesterol levels. People with lipodystrophy, a disorder characterized by particularly severe insulin resistance and dyslipidemia, demonstrated similar abnormalities. Collectively these data from humans with molecularly characterized forms of insulin resistance suggest that partial postreceptor hepatic insulin resistance is a key element in the development of metabolic dyslipidemia and hepatic steatosis.
Figures



Comment in
-
Hoofbeats, zebras, and insights into insulin resistance.J Clin Invest. 2009 Feb;119(2):249-51. doi: 10.1172/jci38420. J Clin Invest. 2009. PMID: 19244606 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
