

The fascia of the limbs and back--a review
- PMID: 19166469
- PMCID: PMC2667913
- DOI: 10.1111/j.1469-7580.2008.01011.x
The fascia of the limbs and back--a review
Abstract
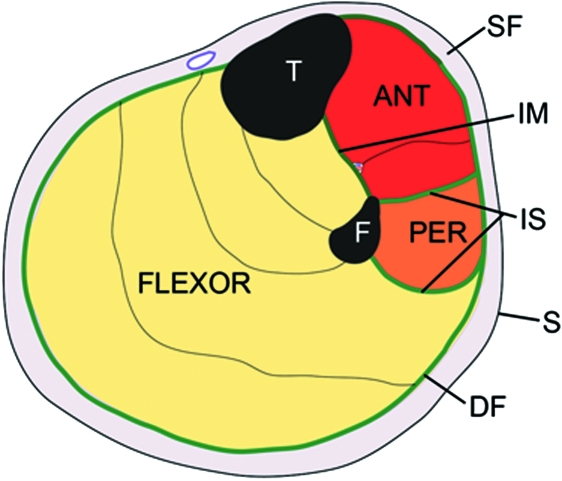
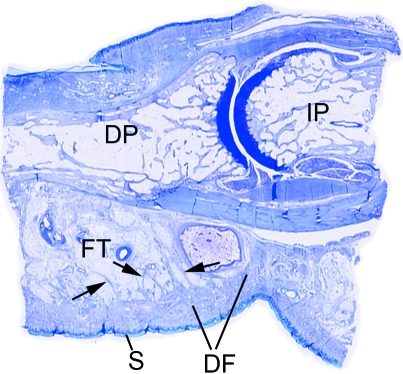
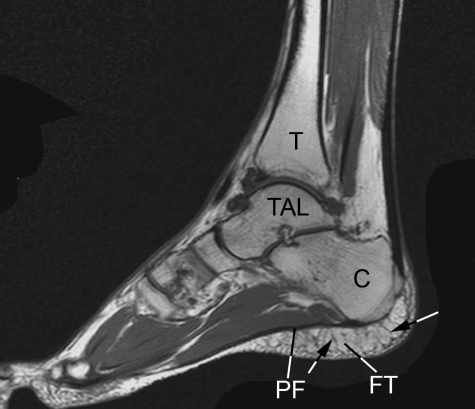
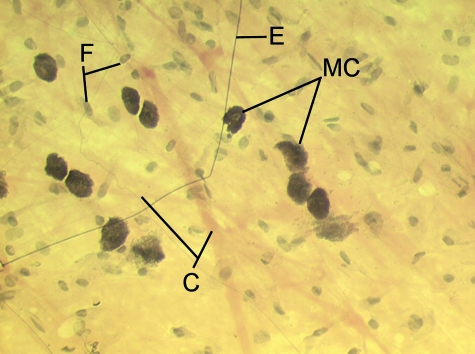
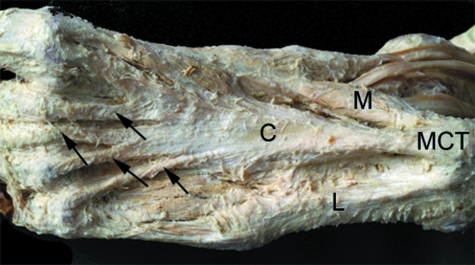
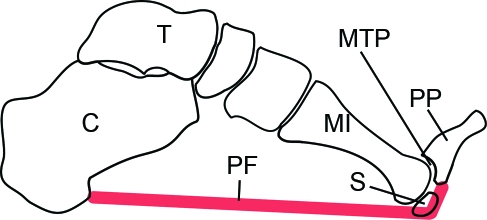
Although fasciae have long interested clinicians in a multitude of different clinical and paramedical disciplines, there have been few attempts to unite the ensuing diverse literature into a single review. The current article gives an anatomical perspective that extends from the gross to the molecular level. For expediency, it deals only with fascia in the limbs and back. Particular focus is directed towards deep fascia and thus consideration is given to structures such as the fascia lata, thoracolumbar fascia, plantar and palmar fascia, along with regional specializations of deep fascia such as retinacula and fibrous pulleys. However, equal emphasis is placed on general aspects of fascial structure and function, including its innervation and cellular composition. Among the many functions of fascia considered in detail are its ectoskeletal role (as a soft tissue skeleton for muscle attachments), its importance for creating osteofascial compartments for muscles, encouraging venous return in the lower limb, dissipating stress concentration at entheses and acting as a protective sheet for underlying structures. Emphasis is placed on recognizing the continuity of fascia between regions and appreciating its key role in coordinating muscular activity and acting as a body-wide proprioceptive organ. Such considerations far outweigh the significance of viewing fascia in a regional context alone.
Figures
References
-
- Abreu MR, Chung CB, Mendes L, Mohana-Borges A, Trudell D, Resnick D. Plantar calcaneal enthesophytes: new observations regarding sites of origin based on radiographic, MR imaging, anatomic, and paleopathologic analysis. Skeletal Radiol. 2003;32:13–21. - PubMed
-
- Abu-Hijleh MF, Harris PF. Deep fascia on the dorsum of the ankle and foot: extensor retinacula revisited. Clin Anat. 2007;20:186–195. - PubMed
-
- Athwal GS, Steinmann SP, Rispoli DM. The distal biceps tendon: footprint and relevant clinical anatomy. J Hand Surg [Am] 2007;32:1225–1229. - PubMed
-
- Augoff K, Kula J, Gosk J, Rutowski R. Epidermal growth factor in Dupuytren's disease. Plast Reconstr Surg. 2005;115:128–133. - PubMed
-
- Augoff K, Ratajczak K, Gosk J, Tabola R, Rutowski R. Gelatinase A activity in Dupuytren's disease. J Hand Surg [Am] 2006;31:1635–1639. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
