

BMI changes during childhood and adolescence as predictors of amount of adult subcutaneous and visceral adipose tissue in men: the GOOD Study
- PMID: 19168597
- PMCID: PMC2661578
- DOI: 10.2337/db08-0606
BMI changes during childhood and adolescence as predictors of amount of adult subcutaneous and visceral adipose tissue in men: the GOOD Study
Abstract
Objective: The amount of visceral adipose tissue is a risk factor for the metabolic syndrome. It is unclear how BMI changes during childhood and adolescence predict adult fat distribution. We hypothesized that there are critical periods during development for the prediction of adult subcutaneous and visceral fat mass by BMI changes during childhood and adolescence.
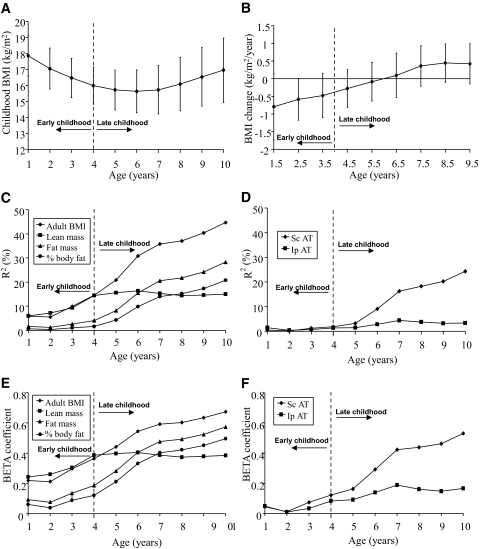
Research design and methods: Detailed growth charts were retrieved for the men participating in the population-based Gothenburg Osteoporosis and Obesity Determinants (GOOD) Study (n = 612). Body composition was analyzed using dual-energy X-ray absorptiometry and adipose tissue areas using abdominal computed tomography at 18 to 20 years of age.
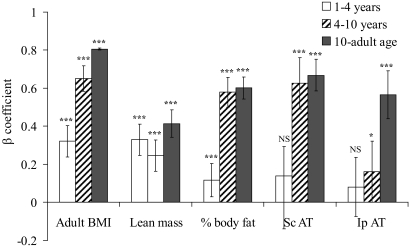
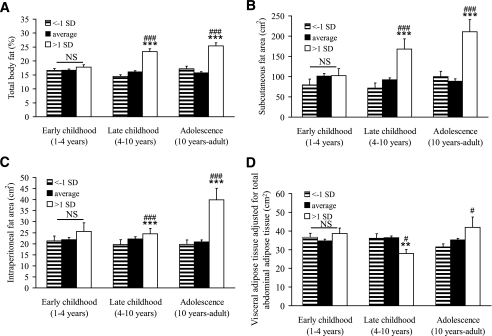
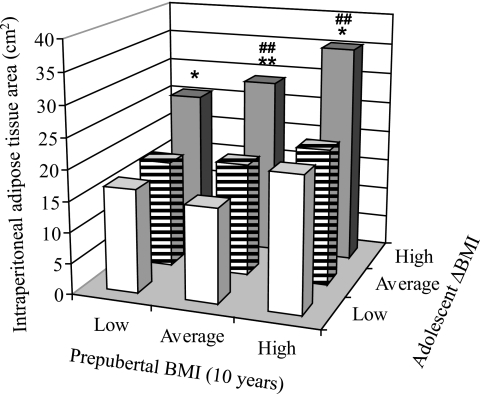
Results: The main finding in the present study was that subjects with increases in BMI Z score of more than 1 SD during adolescence had, independent of prepubertal BMI, both larger subcutaneous (+138%; P < 0.001) and visceral adipose tissue areas (+91%; P < 0.001) than subjects with unchanged BMI Z-score. In contrast, subjects with increases in BMI Z score of more than 1 SD during late childhood had a larger amount of adult subcutaneous adipose tissue (+83%; P < 0.001) than subjects with unchanged BMI Z score but an unaffected amount of visceral adipose tissue. BMI changes during adolescence predict both visceral and subcutaneous adipose tissue of the abdomen, whereas BMI changes during late childhood predict only the subcutaneous adipose tissue.
Conclusions: The amount of visceral adipose tissue in young adult men was associated with BMI changes specifically during adolescence, whereas the amount of subcutaneous adipose tissue was associated with BMI changes during both late childhood and adolescence.
Figures
References
-
- Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, Allen K, Lopes M, Savoye M, Morrison J, Sherwin RS, Caprio S: Obesity and the metabolic syndrome in children and adolescents. N Engl J Med 350: 2362– 2374, 2004 - PubMed
-
- Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM: Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. JAMA 291: 2847– 2850, 2004 - PubMed
-
- Arsenault BJ, Lachance D, Lemieux I, Almeras N, Tremblay A, Bouchard C, Perusse L, Despres JP: Visceral adipose tissue accumulation, cardiorespiratory fitness, and features of the metabolic syndrome. Arch Intern Med 167: 1518– 1525, 2007 - PubMed
-
- Goodpaster BH, Krishnaswami S, Harris TB, Katsiaras A, Kritchevsky SB, Simonsick EM, Nevitt M, Holvoet P, Newman AB: Obesity, regional body fat distribution, and the metabolic syndrome in older men and women. Arch Intern Med 165: 777– 783, 2005 - PubMed
-
- Fox CS, Massaro JM, Hoffmann U, Pou KM, Maurovich-Horvat P, Liu CY, Vasan RS, Murabito JM, Meigs JB, Cupples LA, D'Agostino RB, Sr, O'Donnell CJ: Abdominal visceral and subcutaneous adipose tissue compartments. Association with metabolic risk factors in the Framingham Heart Study. Circulation 116: 39– 48, 2007 - PubMed
