

Trichostatin a inhibits corneal haze in vitro and in vivo
- PMID: 19168895
- PMCID: PMC3711114
- DOI: 10.1167/iovs.08-2919
Trichostatin a inhibits corneal haze in vitro and in vivo
Abstract
Purpose: Trichostatin A (TSA), a histone deacetylase inhibitor, has been shown to suppress TGF-beta-induced fibrogenesis in many nonocular tissues. The authors evaluated TSA cytotoxicity and its antifibrogenic activity on TGF-beta-driven fibrosis in the cornea with the use of in vitro and in vivo models.
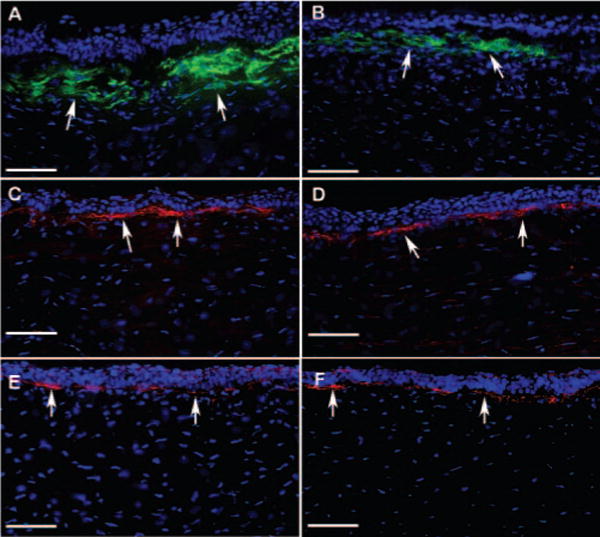
Methods: Human corneal fibroblasts (HSFs) were used for in vitro studies, and New Zealand White rabbits were used for in vivo studies. Haze in the rabbit cornea was produced with photorefractive keratectomy (PRK) using excimer laser. Trypan blue exclusion and MTT assays evaluated TSA cytotoxicity to the cornea. Density of haze in the rabbit eye was graded with slit lamp biomicroscopy. Real-time PCR, immunoblotting, or immunocytochemistry was used to measure alpha-smooth muscle actin (SMA), fibronectin, and collagen type IV mRNA or protein levels. TUNEL assay was used to detect cell death.
Results: TSA concentrations of 250 nM or less were noncytotoxic and did not alter normal HSF morphology or proliferation. TGF-beta1 treatment of HSF significantly increased mRNA and protein levels of SMA (9-fold), fibronectin (2.5-fold), and collagen type IV (2-fold). TSA treatment showed 60% to 75% decreases in TGF-beta1-induced SMA and fibronectin mRNA levels and 1.5- to 3.0-fold decreases in protein levels but had no effect on collagen type IV mRNA or protein levels in vitro. Two-minute topical treatment of TSA on rabbit corneas subjected to -9 D PRK significantly decreased corneal haze in vivo.
Conclusions: TSA inhibits TGF-beta1-induced accumulation of extracellular matrix and myofibroblast formation in the human cornea in vitro and markedly decreases haze in rabbit cornea in vivo.
Figures






References
-
- Fong CS. Refractive surgery: the future of perfect vision? Singapore Med J. 2007;48:709–718. - PubMed
-
- Melki SA, Azar DT. LASIK complications: etiology, management, and prevention. Surv Ophthalmol. 2001;46:95–116. - PubMed
-
- McDonnell PJ. Emergence of refractive surgery. Arch Ophthalmol. 2000;118:1119–11120. - PubMed
-
- Shortt AJ, Bunce C, Allan BD. Evidence for superior efficacy and safety of LASIK over photorefractive keratectomy for correction of myopia. Ophthalmology. 2006;113:1897–1908. - PubMed
-
- Lee JB, Kim JS, Choe C, Seong GJ, Kim EK. Comparison of two procedures: photorefractive keratectomy versus laser in situ keratomileusis for low to moderate myopia. Jpn J Ophthalmol. 2001;45:487–491. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
