

Bone marrow lesions from osteoarthritis knees are characterized by sclerotic bone that is less well mineralized
- PMID: 19171047
- PMCID: PMC2688243
- DOI: 10.1186/ar2601
Bone marrow lesions from osteoarthritis knees are characterized by sclerotic bone that is less well mineralized
Abstract
Introduction: Although the presence of bone marrow lesions (BMLs) on magnetic resonance images is strongly associated with osteoarthritis progression and pain, the underlying pathology is not well established. The aim of the present study was to evaluate the architecture of subchondral bone in regions with and without BMLs from the same individual using bone histomorphometry.
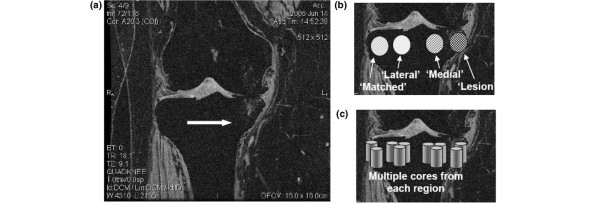
Methods: Postmenopausal female subjects (n = 6, age 48 to 90 years) with predominantly medial compartment osteoarthritis and on a waiting list for total knee replacement were recruited. To identify the location of the BMLs, subjects had a magnetic resonance imaging scan performed on their study knee prior to total knee replacement using a GE 1.5 T scanner with a dedicated extremity coil. An axial map of the tibial plateau was made, delineating the precise location of the BML. After surgical removal of the tibial plateau, the BML was localized using the axial map from the magnetic resonance image and the lesion excised along with a comparably sized bone specimen adjacent to the BML and from the contralateral compartment without a BML. Cores were imaged via microcomputed tomography, and the bone volume fraction and tissue mineral density were calculated for each core. In addition, the thickness of the subchondral plate was measured, and the following quantitative metrics of trabecular structure were calculated for the subchondral trabecular bone in each core: trabecular number, thickness, and spacing, structure model index, connectivity density, and degree of anisotropy. We computed the mean and standard deviation for each parameter, and the unaffected bone from the medial tibial plateau and the bone from the lateral tibial plateau were compared with the affected BML region in the medial tibial plateau.
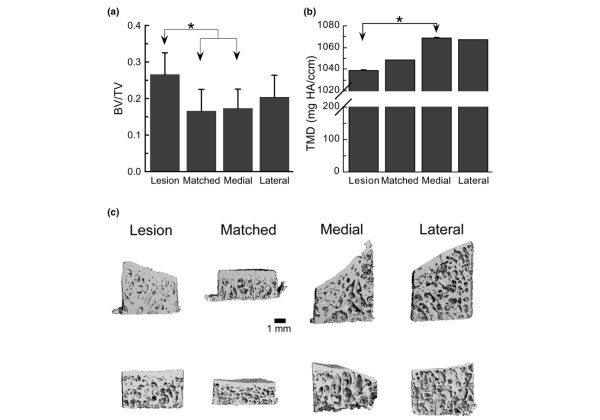
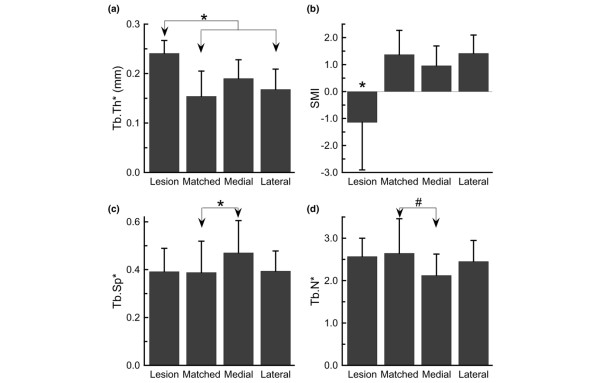
Results: Cores from the lesion area displayed increased bone volume fraction but reduced tissue mineral density. The samples from the subchondral trabecular lesion area exhibited increased trabecular thickness and were also markedly more plate-like than the bone in the other three locations, as evidenced by the lower value of the structural model index. Other differences in structure that were noted were increased trabecular spacing and a trend towards decreased trabecular number in the cores from the medial location as compared with the contralateral location.
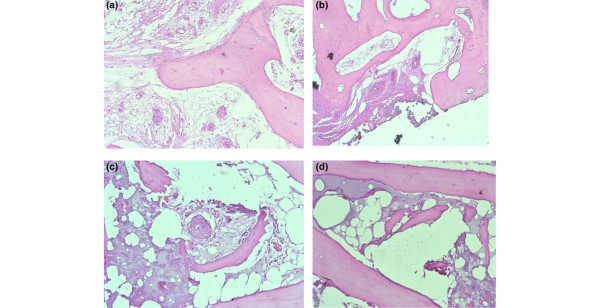
Conclusions: Our preliminary data localize specific changes in bone mineralization, remodeling and defects within BMLs features that are adjacent to the subchondral plate. These BMLs appear to be sclerotic compared with unaffected regions from the same individual based on the increased bone volume fraction and increased trabecular thickness. The mineral density in these lesions, however, is reduced and may render this area to be mechanically compromised, and thus susceptible to attrition.
Figures
Similar articles
-
Raman microspectroscopy demonstrates reduced mineralization of subchondral bone marrow lesions in knee osteoarthritis patients.Bone Rep. 2020 Apr 22;12:100269. doi: 10.1016/j.bonr.2020.100269. eCollection 2020 Jun. Bone Rep. 2020. PMID: 32395569 Free PMC article.
-
Greater heterogeneity of the bone mineralisation density distribution and low bone matrix mineralisation characterise tibial subchondral bone marrow lesions in knee osteoarthritis patients.Bone. 2021 Aug;149:115979. doi: 10.1016/j.bone.2021.115979. Epub 2021 Apr 27. Bone. 2021. PMID: 33915332
-
Bone marrow lesions are associated with altered trabecular morphometry.Osteoarthritis Cartilage. 2012 Dec;20(12):1519-26. doi: 10.1016/j.joca.2012.08.013. Epub 2012 Aug 30. Osteoarthritis Cartilage. 2012. PMID: 22940708 Free PMC article.
-
The Significance of Osteoarthritis-associated Bone Marrow Lesions in the Knee.J Am Acad Orthop Surg. 2019 Oct 15;27(20):752-759. doi: 10.5435/JAAOS-D-18-00267. J Am Acad Orthop Surg. 2019. PMID: 30964755 Review.
-
MRI-detected subchondral bone marrow signal alterations of the knee joint: terminology, imaging appearance, relevance and radiological differential diagnosis.Osteoarthritis Cartilage. 2009 Sep;17(9):1115-31. doi: 10.1016/j.joca.2009.03.012. Epub 2009 Mar 31. Osteoarthritis Cartilage. 2009. PMID: 19358902 Review.
Cited by
-
Clinical significance of bone changes in osteoarthritis.Ther Adv Musculoskelet Dis. 2012 Aug;4(4):259-67. doi: 10.1177/1759720X12437354. Ther Adv Musculoskelet Dis. 2012. PMID: 22859925 Free PMC article.
-
Surgical Treatment of Insufficiency Fractures of the Knee.Arthrosc Tech. 2019 Oct 11;8(11):e1327-e1332. doi: 10.1016/j.eats.2019.07.008. eCollection 2019 Nov. Arthrosc Tech. 2019. PMID: 31890503 Free PMC article.
-
Osteoblast-chondrocyte interactions in osteoarthritis.Curr Osteoporos Rep. 2014 Mar;12(1):127-34. doi: 10.1007/s11914-014-0192-5. Curr Osteoporos Rep. 2014. PMID: 24458429 Free PMC article. Review.
-
Raman microspectroscopy demonstrates reduced mineralization of subchondral bone marrow lesions in knee osteoarthritis patients.Bone Rep. 2020 Apr 22;12:100269. doi: 10.1016/j.bonr.2020.100269. eCollection 2020 Jun. Bone Rep. 2020. PMID: 32395569 Free PMC article.
-
Subchondral bone remodelling in osteoarthritis.EFORT Open Rev. 2019 Jun 3;4(6):221-229. doi: 10.1302/2058-5241.4.180102. eCollection 2019 Jun. EFORT Open Rev. 2019. PMID: 31210964 Free PMC article. Review.
References
-
- Felson DT, Chaisson CE, Hill CL, Totterman SM, Gale ME, Skinner KM, Kazis L, Gale DR. The association of bone marrow lesions with pain in knee osteoarthritis [see comments] Ann Intern Med. 2001;134:541–549. - PubMed
-
- Felson DT, McLaughlin S, Goggins J, LaValley MP, Gale ME, Totterman S, Li W, Hill CL, Gale DR. Bone marrow edema and its relation to progression of knee osteoarthritis. Ann Intern Med. 2003;139:330–336. - PubMed
-
- Zanetti M, Bruder E, Romero J, Hodler J. Bone marrow edema pattern in osteoarthritic knees: correlation between MR imaging and histologic findings. Radiology. 2000;215:835–840. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
