

Recovery of birth weight z score within 2 years of diagnosis is positively associated with pulmonary status at 6 years of age in children with cystic fibrosis
- PMID: 19171643
- PMCID: PMC2775492
- DOI: 10.1542/peds.2007-3089
Recovery of birth weight z score within 2 years of diagnosis is positively associated with pulmonary status at 6 years of age in children with cystic fibrosis
Abstract
Objective: We recently reported that 60% of children newly diagnosed with cystic fibrosis who had pancreatic insufficiency responded to treatment initiation and achieved catch-up weight gain to a level comparable with their birth weight z score within 2 years of diagnosis ("responders"), whereas the remaining 40% failed to do so ("nonresponders"). The present study examined the impact of this early weight recovery on subsequent growth pattern and pulmonary status at 6 years of age.
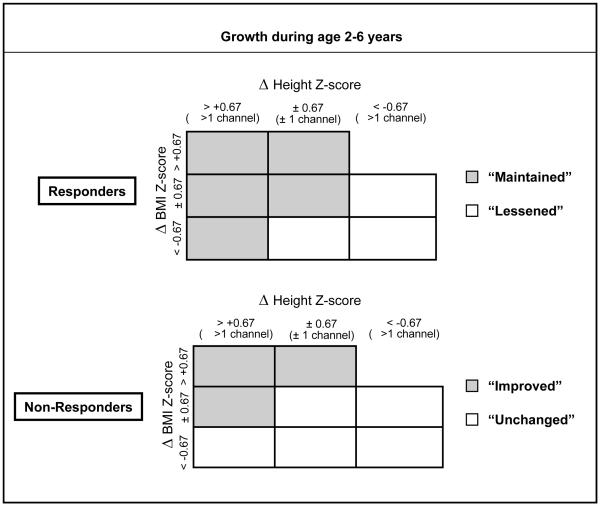
Patients and methods: Sixty-three children with cystic fibrosis who had pancreatic insufficiency but no meconium ileus, and were enrolled in the Wisconsin Cystic Fibrosis Neonatal Screening Project, were studied. Responders were defined by a recovery of weight z score comparable with that at birth within 2 years of diagnosis. From ages 2 to 6, growth was measured by both height and BMI. Pulmonary status was evaluated by symptoms, spirometry, quantitative chest radiography, and respiratory microbiology.
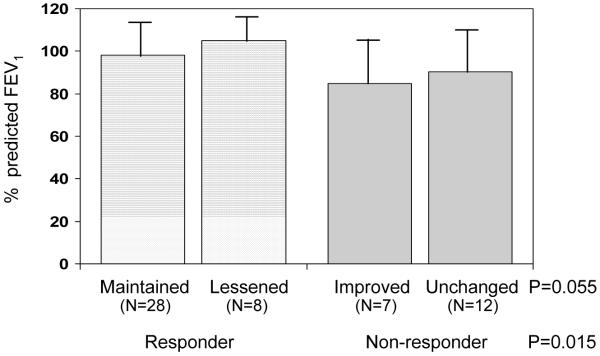
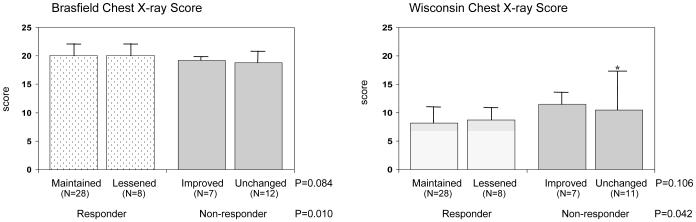
Results: The majority (71%) of the responders maintained their early weight recovery through 6 years of age, whereas only 32% of the nonresponders achieved substantial growth improvement from 2 to 6 years of age. Proportionately fewer responders reported cough symptoms (10% daytime cough; 22% nighttime cough) compared with nonresponders (41% daytime cough; 45% nighttime cough) at age 6. The percentage of predicted forced expiratory volume in 1 second at age 6 was 11% higher in responders (99.5% +/- 13.9%) compared with nonresponders (88.3% +/- 18.5%). Responders had significantly better Brasfield (20.1 +/- 1.4) and Wisconsin chest radiograph (8.3 +/- 3.3) scores compared with nonresponders (Brasfield: 18.9 +/- 1.8; Wisconsin: 12.3 +/- 8.3). Respiratory microbiology results were not significantly different. Multiple regression analyses indicated that the positive association between responder and percent predicted forced expiratory volume in 1 second at 6 years of age remained statistically significant after controlling for infections with Pseudomonas aeruginosa and Staphylococcus aureus and chest radiograph scores. Growth patterns from 2 to 6 years of age were not associated with pulmonary measures at age 6.
Conclusions: Patients with cystic fibrosis with pancreatic insufficiency who achieved early growth recovery within 2 years of diagnosis had fewer cough symptoms, higher lung function, and better chest radiograph scores at 6 years of age.
Figures
References
-
- Kraemer R, Rudeberg A, Hadorn B, Rossie E. Relative underweight in cystic fibrosis and its prognostic value. Acta Paediatr Scand. 1978;67:33–7. - PubMed
-
- Giglio L, Candusso M, D’Orazio C, Mastella G, Faraguna D. Failure to thrive: the earliest feature of cystic fibrosis in infants diagnosed by neonatal screening. Acta Paediatrica. 1997;86:1162–5. - PubMed
-
- Lai HC, Kosorok MR, Sondel SA, Chen ST, FitzSimmons SC, Green CG, Shen G, Walker S, Farrell PM. Growth status in children with cystic fibrosis based on the National Cystic Fibrosis Patient Registry data: evaluation of various criteria used to identify malnutrition. J Pediatr. 1998;132:478–85. - PubMed
-
- McNaughton SA, Stormont DA, Shepherd RW, Francis PW, Dean B. Growth failure in cystic fibrosis. J Paediatr Child Health. 1999;35:86–92. - PubMed
-
- Cystic Fibrosis Foundation . Cystic Fibrosis Foundation Patient Registry Annual Data Report 2002. Cystic Fibrosis Foundation; Bethesda, MD: 2003.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
