

Sensitivity of surveillance studies for detecting asymptomatic and unsuspected relapse of high-risk neuroblastoma
- PMID: 19171710
- PMCID: PMC2667809
- DOI: 10.1200/JCO.2008.17.6107
Sensitivity of surveillance studies for detecting asymptomatic and unsuspected relapse of high-risk neuroblastoma
Abstract
Purpose: Relapse-free survival (RFS) is a powerful measure of treatment efficacy. We describe the sensitivity of standard surveillance studies for detecting relapse of neuroblastoma (NB).
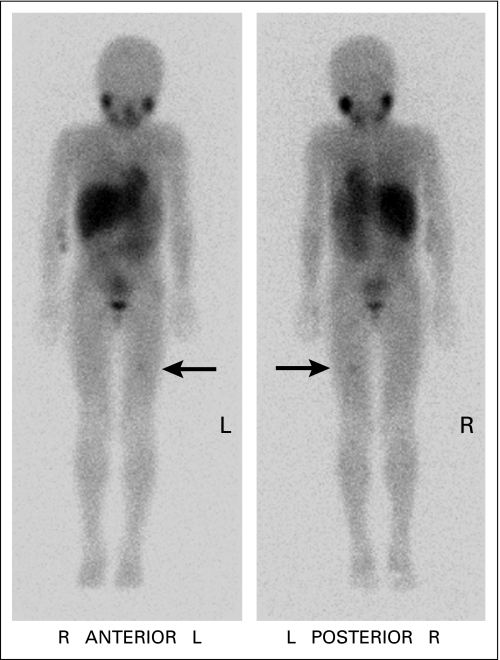
Patients and methods: The patients were in complete/very good partial remission of high-risk NB; routine monitoring revealed asymptomatic and, therefore, unsuspected relapses in 113 patients, whereas 41 patients had symptoms prompting urgent evaluations. Assessments every 2 to 4 months included computed tomography, iodine-131-metaiodobenzylguanidine (131)I-MIBG; through November 1999) or iodine-123-metaiodobenzylguanidine ((123)I-MIBG) scan, urine catecholamines, and bone marrow (BM) histology. Bone scan was routine through 2002.
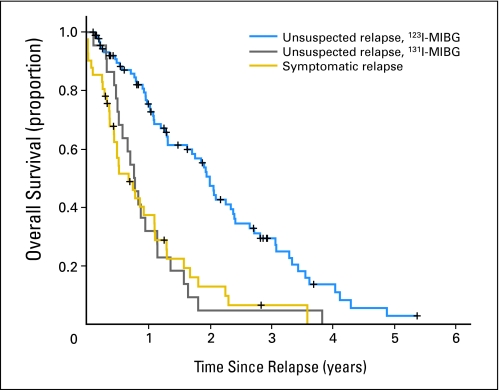
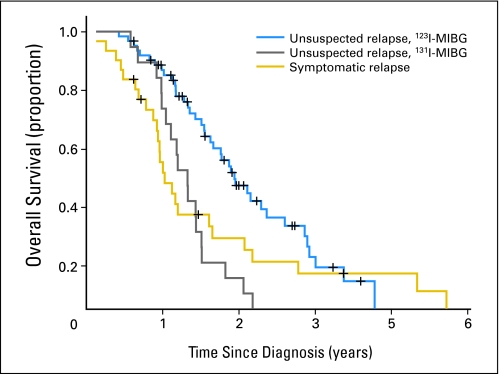
Results: (123)I-MIBG scan was the most reliable study for revealing unsuspected relapse; it had an 82% detection rate, which was superior to the rates with (131)I-MIBG scan (64%; P = .1), bone scan (36%; P < .001), and BM histology (34%; P < .001). Among asymptomatic patients, (123)I-MIBG scan was the sole positive study indicating relapse in 25 (27%) of 91 patients compared with one (4.5%) of 22 patients for (131)I-MIBG scan (P = .04) and 0% to 6% of patients for each of the other studies (P < .001). Patients whose monitoring included (123)I-MIBG scan were significantly less likely than patients monitored by (131)I-MIBG scan to have an extensive osteomedullary relapse and had a significantly longer survival from relapse (P < .001) and from diagnosis (P = .002). They also had significantly longer survival than patients with symptomatic relapses (P = .002).
Conclusion: (123)I-MIBG scan is essential for valid estimation of the duration of RFS of patients with high-risk NB. Without monitoring that includes (123)I-MIBG scan, caution should be used when comparing RFS between institutions and protocols.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
False-positive MIBG scans with normal computed tomography imaging in patients with high-risk neuroblastoma.J Clin Oncol. 2009 Dec 1;27(34):e233-4; author reply e235. doi: 10.1200/JCO.2009.24.0036. Epub 2009 Nov 2. J Clin Oncol. 2009. PMID: 19884537 No abstract available.
Similar articles
-
Impact of metaiodobenzylguanidine scintigraphy on assessing response of high-risk neuroblastoma to dose-intensive induction chemotherapy.J Clin Oncol. 2003 Mar 15;21(6):1082-6. doi: 10.1200/JCO.2003.07.142. J Clin Oncol. 2003. PMID: 12637474
-
The role of 131 iodine-metaiodobenzylguanidine scanning in the correlative imaging of patients with neuroblastoma.Pediatrics. 1996 Feb;97(2):246-50. Pediatrics. 1996. PMID: 8584386
-
Metastatic neuroblastoma in children older than one year: prognostic significance of the initial metaiodobenzylguanidine scan and proposal for a scoring system.Cancer. 1996 Feb 15;77(4):805-11. doi: 10.1002/(sici)1097-0142(19960215)77:4<805::aid-cncr29>3.0.co;2-3. Cancer. 1996. PMID: 8616776
-
Criteria for evaluation of disease extent by (123)I-metaiodobenzylguanidine scans in neuroblastoma: a report for the International Neuroblastoma Risk Group (INRG) Task Force.Br J Cancer. 2010 Apr 27;102(9):1319-26. doi: 10.1038/sj.bjc.6605621. Br J Cancer. 2010. PMID: 20424613 Free PMC article. Review.
-
Meta-iodobenzylguanidine in children.Semin Nucl Med. 1993 Jul;23(3):231-42. doi: 10.1016/s0001-2998(05)80104-7. Semin Nucl Med. 1993. PMID: 8378796 Review.
Cited by
-
Radiomics models to predict bone marrow metastasis of neuroblastoma using CT.Cancer Innov. 2024 Jun 28;3(5):e135. doi: 10.1002/cai2.135. eCollection 2024 Oct. Cancer Innov. 2024. PMID: 38948899 Free PMC article.
-
Norepinephrine Transporter as a Target for Imaging and Therapy.J Nucl Med. 2017 Sep;58(Suppl 2):39S-53S. doi: 10.2967/jnumed.116.186833. J Nucl Med. 2017. PMID: 28864611 Free PMC article. Review.
-
Imaging in childhood cancer: a Society for Pediatric Radiology and Children's Oncology Group Joint Task Force report.Pediatr Blood Cancer. 2013 Aug;60(8):1253-60. doi: 10.1002/pbc.24533. Epub 2013 Apr 9. Pediatr Blood Cancer. 2013. PMID: 23572212 Free PMC article. Review.
-
Striking dichotomy in outcome of MYCN-amplified neuroblastoma in the contemporary era.Cancer. 2014 Jul 1;120(13):2050-9. doi: 10.1002/cncr.28687. Epub 2014 Apr 1. Cancer. 2014. PMID: 24691684 Free PMC article.
-
Phase I trial of a bivalent gangliosides vaccine in combination with β-glucan for high-risk neuroblastoma in second or later remission.Clin Cancer Res. 2014 Mar 1;20(5):1375-82. doi: 10.1158/1078-0432.CCR-13-1012. Epub 2014 Feb 11. Clin Cancer Res. 2014. PMID: 24520094 Free PMC article. Clinical Trial.
References
-
- Dubois SG, Kalika Y, Lukens JN, et al. Metastatic sites in stage IV and IVS neuroblastoma correlate with age, tumor biology, and survival. J Pediatr Hematol Oncol. 1999;21:181–189. - PubMed
-
- Kushner BH. Neuroblastoma: A disease requiring a multitude of imaging studies. J Nucl Med. 2004;45:1172–1188. - PubMed
-
- Brodeur GM, Pritchard J, Berthold F, et al. Revisions of the international criteria for neuroblastoma diagnosis, staging, and response to treatment. J Clin Oncol. 1993;11:1466–1477. - PubMed
-
- Kushner BH, Yeh SDJ, Kramer K, et al. Impact of MIBG scintigraphy on assessing response of high-risk neuroblastoma to dose-intensive induction chemotherapy. J Clin Oncol. 2003;21:1082–1086. - PubMed
-
- Preacher KJ. Calculation for the chi-square test: An interactive calculation tool for chi-square tests of goodness of fit and independence. http://www.quantpsy.org.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
