

Congruence between NOTCH3 mutations and GOM in 131 CADASIL patients
- PMID: 19174371
- PMCID: PMC2668941
- DOI: 10.1093/brain/awn364
Congruence between NOTCH3 mutations and GOM in 131 CADASIL patients
Abstract
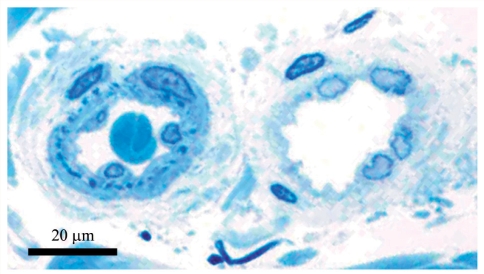
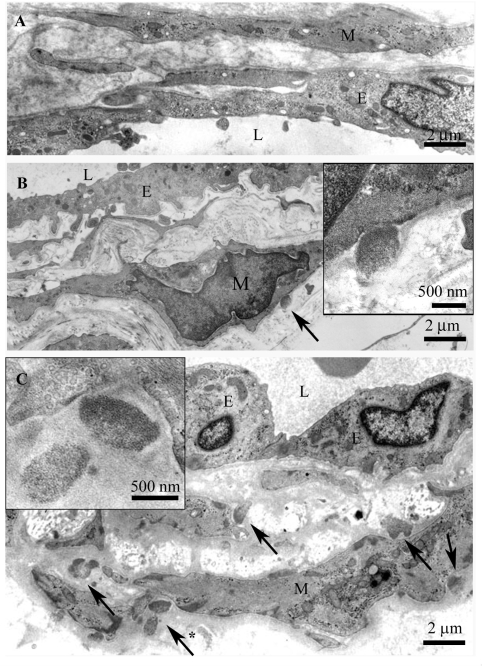
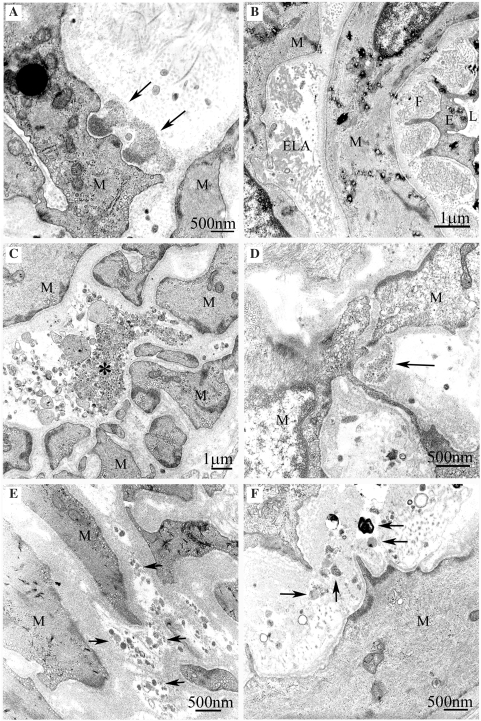
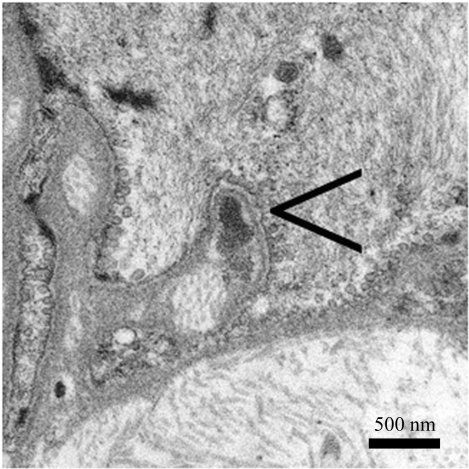
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is the most common hereditary subcortical vascular dementia. It is caused by mutations in NOTCH3 gene, which encodes a large transmembrane receptor Notch3. The key pathological finding is the accumulation of granular osmiophilic material (GOM), which contains extracellular domains of Notch3, on degenerating vascular smooth muscle cells (VSMCs). GOM has been considered specifically diagnostic for CADASIL, but the reports on the sensitivity of detecting GOM in patients' skin biopsy have been contradictory. To solve this contradiction, we performed a retrospective investigation of 131 Finnish, Swedish and French CADASIL patients, who had been adequately examined for both NOTCH3 mutation and presence of GOM. The patients were examined according to the diagnostic practice in each country. NOTCH3 mutations were assessed by restriction enzyme analysis of specific mutations or by sequence analysis. Presence of GOM was examined by electron microscopy (EM) in skin biopsies. Biopsies of 26 mutation-negative relatives from CADASIL families served as the controls. GOM was detected in all 131 mutation positive patients. Altogether our patients had 34 different pathogenic mutations which included three novel point mutations (p.Cys67Ser, p.Cys251Tyr and p.Tyr1069Cys) and a novel duplication (p.Glu434_Leu436dup). The detection of GOM by EM in skin biopsies was a highly reliable diagnostic method: in this cohort the congruence between NOTCH3 mutations and presence of GOM was 100%. However, due to the retrospective nature of this study, exact figure for sensitivity cannot be determined, but it would require a prospective study to exclude possible selection bias. The identification of a pathogenic NOTCH3 mutation is an indisputable evidence for CADASIL, but demonstration of GOM provides a cost-effective guide for estimating how far one should proceed with the extensive search for a new or an uncommon mutations among the presently known over 170 different NOTCH3 gene defects. The diagnostic skin biopsy should include the border zone between deep dermis and upper subcutis, where small arterial vessels of correct size are located. Detection of GOM requires technically adequate biopsies and distinction of true GOM from fallacious deposits. If GOM is not found in the first vessel or biopsy, other vessels or additional biopsies should be examined.
Figures
References
-
- Baudrimont M, Dubas F, Joutel A, Tournier-Lasserve E, Bousser MG. Autosomal dominant leukoencephalopathy and subcortical ischemic stroke. A clinicopathological study. Stroke. 1993;24:122–5. - PubMed
-
- Brulin P, Godfraind C, Leteurtre E, Ruchoux MM. Morphometric analysis of ultrastructural vascular changes in CADASIL: analysis of 50 skin biopsy specimens and pathogenic implications. Acta Neuropathol (Berl) 2002;104:241–8. - PubMed
-
- Dichgans M. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy: phenotypic and mutational spectrum. J Neurol Sci. 2002;203–4:77–80. - PubMed
-
- Dichgans M, Ludwig H, Muller-Hocker J, Messerschmidt A, Gasser T. Small in-frame deletions and missense mutations in CADASIL: 3D models predict misfolding of Notch3 EGF-like repeat domains. Eur J Hum Genet. 2000;8:280–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
