

Dose calculation with respiration-averaged CT processed from cine CT without a respiratory surrogate
- PMID: 19175131
- PMCID: PMC3910265
- DOI: 10.1118/1.3015197
Dose calculation with respiration-averaged CT processed from cine CT without a respiratory surrogate
Abstract
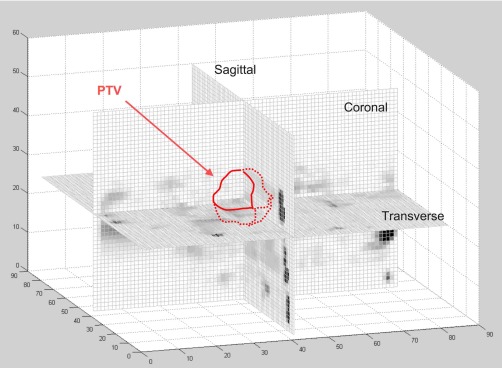
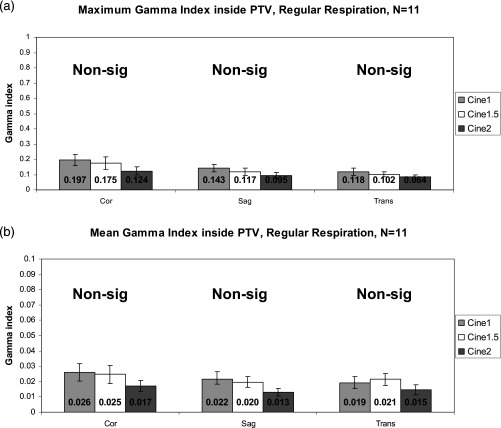
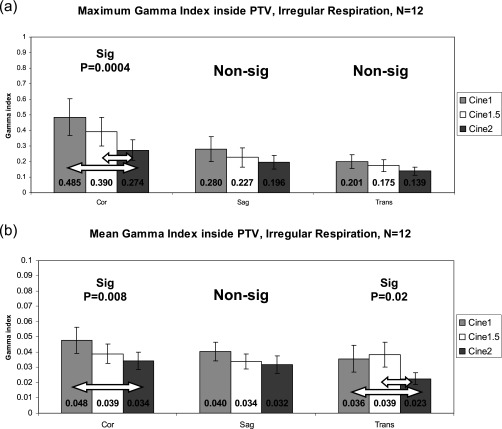
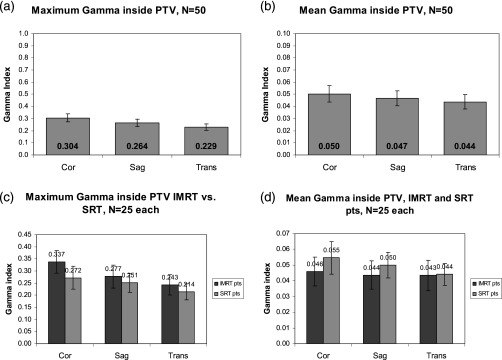
Dose calculation for thoracic radiotherapy is commonly performed on a free-breathing helical CT despite artifacts caused by respiratory motion. Four-dimensional computed tomography (4D-CT) is one method to incorporate motion information into the treatment planning process. Some centers now use the respiration-averaged CT (RACT), the pixel-by-pixel average of the ten phases of 4D-CT, for dose calculation. This method, while sparing the tedious task of 4D dose calculation, still requires 4D-CT technology. The authors have recently developed a means to reconstruct RACT directly from unsorted cine CT data from which 4D-CT is formed, bypassing the need for a respiratory surrogate. Using RACT from cine CT for dose calculation may be a means to incorporate motion information into dose calculation without performing 4D-CT. The purpose of this study was to determine if RACT from cine CT can be substituted for RACT from 4D-CT for the purposes of dose calculation, and if increasing the cine duration can decrease differences between the dose distributions. Cine CT data and corresponding 4D-CT simulations for 23 patients with at least two breathing cycles per cine duration were retrieved. RACT was generated four ways: First from ten phases of 4D-CT, second, from 1 breathing cycle of images, third, from 1.5 breathing cycles of images, and fourth, from 2 breathing cycles of images. The clinical treatment plan was transferred to each RACT and dose was recalculated. Dose planes were exported at orthogonal planes through the isocenter (coronal, sagittal, and transverse orientations). The resulting dose distributions were compared using the gamma index within the planning target volume (PTV). Failure criteria were set to 2%/1 mm. A follow-up study with 50 additional lung cancer patients was performed to increase sample size. The same dose recalculation and analysis was performed. In the primary patient group, 22 of 23 patients had 100% of points within the PTV pass y criteria. The average maximum and mean y indices were very low (well below 1), indicating good agreement between dose distributions. Increasing the cine duration generally increased the dose agreement. In the follow-up study, 49 of 50 patients had 100% of points within the PTV pass the y criteria. The average maximum and mean y indices were again well below 1, indicating good agreement. Dose calculation on RACT from cine CT is negligibly different from dose calculation on RACT from 4D-CT. Differences can be decreased further by increasing the cine duration of the cine CT scan.
Figures




References
-
- D’Souza W. D. et al., “The use of gated and 4D CT imaging in planning for stereotactic body radiation therapy,” Med. Dosim. ZZZZZZ 32, 92–101 (2007). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
