

Human papillomavirus type 18 DNA load and 2-year cumulative diagnoses of cervical intraepithelial neoplasia grades 2-3
- PMID: 19176451
- PMCID: PMC2724855
- DOI: 10.1093/jnci/djn461
Human papillomavirus type 18 DNA load and 2-year cumulative diagnoses of cervical intraepithelial neoplasia grades 2-3
Abstract
Background: The clinical relevance of the amount of human papillomavirus type 18 (HPV18) DNA in cervical tissue (ie, HPV18 DNA load) is unknown.
Methods: Study subjects were 303 women who were HPV18 positive at enrollment into the Atypical Squamous Cells of Undetermined Significance (ASC-US) and Low-Grade Squamous Intraepithelial Lesion (LSIL) Triage Study. HPV18 DNA load, expressed as copies of HPV18 per nanogram of cellular DNA, at enrollment was quantitatively measured. Subjects were followed up semiannually for a period of 2 years for detection of cervical intraepithelial neoplasia 2-3 (CIN2-3). A linear regression model was used to examine associations of CIN2-3 with HPV18 DNA load. All statistical tests were two-sided.
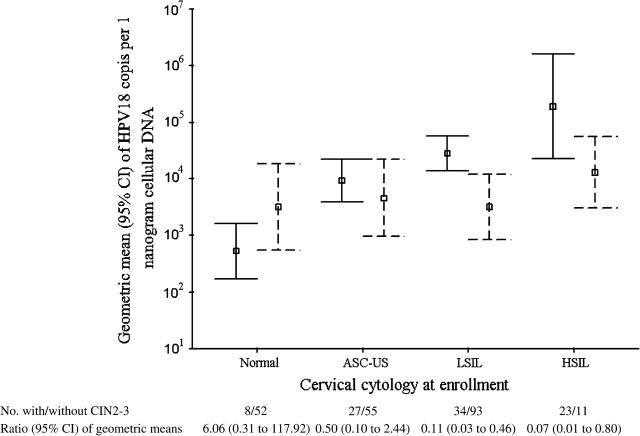
Results: CIN2-3 was confirmed in 92 of 303 (30.4%) HPV18-positive women. Among women without CIN2-3, HPV18 DNA load was positively associated with increasing severity of cervical cytology at enrollment (Ptrend < .001). However, among those with CIN2-3, HPV18 DNA load was not associated with severity of cervical cytology at enrollment (Ptrend = .33). The ratios of geometric means of HPV18 DNA load at enrollment among women with CIN2-3, relative to those without, were 6.06 (95% confidence interval [CI] = 0.31 to 117.92) for those with normal cytology at enrollment, 0.50 (95% CI = 0.10 to 2.44) for those with ASC-US, 0.11 (95% CI = 0.03 to 0.46) for those with LSIL, and 0.07 (95% CI = 0.01 to 0.80) for those with high-grade squamous intraepithelial lesion (HSIL). After adjusting for age and coinfection with other high-risk HPVs, a statistically significant association of lower HPV18 DNA load with CIN2-3 was observed among women with LSIL or HSIL at enrollment (P = .02). Within the 2-year period, HPV18 DNA load was unrelated to the timing of CIN2-3 diagnosis. Overall results were similar when the outcome was CIN3.
Conclusions: HPV18 DNA load was higher for women with LSIL or HSIL at enrollment with no evidence of CIN2-3 during the 2-year follow-up period than it was for women with CIN2-3. Thus, testing for high levels of HPV18 DNA does not appear to be clinically useful.
Figures
Comment in
-
Prognostic value of measuring load of human papillomavirus DNA in cervical samples: an elusive target.J Natl Cancer Inst. 2009 Feb 4;101(3):131-3. doi: 10.1093/jnci/djn486. Epub 2009 Jan 27. J Natl Cancer Inst. 2009. PMID: 19176455 No abstract available.
References
-
- Munoz N, Bosch FX, de Sanjose S, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348(6):518–527. - PubMed
-
- Smith JS, Lindsay L, Hoots B, et al. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer. 2007;121(3):621–632. - PubMed
-
- Woodman CB, Collins S, Rollason TP, et al. Human papillomavirus type 18 and rapidly progressing cervical intraepithelial neoplasia. Lancet. 2003;361(9351):40–43. - PubMed
-
- Kurman RJ, Schiffman MH, Lancaster WD, et al. Analysis of individual human papillomavirus types in cervical neoplasia: a possible role for type 18 in rapid progression. Am J Obstet Gynecol. 1988;159(2):293–296. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
