

Neutrophil gelatinase-associated lipocalin (NGAL) and progression of chronic kidney disease
- PMID: 19176795
- PMCID: PMC2637601
- DOI: 10.2215/CJN.03530708
Neutrophil gelatinase-associated lipocalin (NGAL) and progression of chronic kidney disease
Abstract
Background and objectives: Chronic kidney disease (CKD) has recently assumed epidemic proportion, becoming a troubling emerging cause of morbidity, especially if it progresses to terminal stage (ESRD). The authors aimed to evaluate whether neutrophil gelatinase-associated lipocalin (NGAL), a novel specific biomarker of acute kidney injury, could predict the progression of CKD.
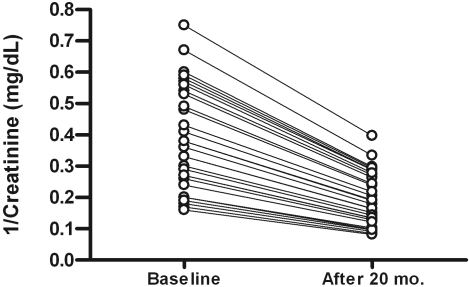
Design, setting, participants, & measurements: Serum and urinary NGAL levels, together with a series of putative progression factors, were evaluated in a cohort of 96 patients (mean age: 57 +/- 16 years) affected by nonterminal CKD (eGFR > or =15 ml/min/1.73 m(2)) of various etiology. Progression of CKD, assessed as doubling of baseline serum creatinine and/or onset of ESRD, was evaluated during follow-up.
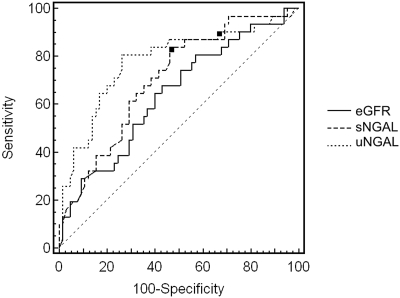
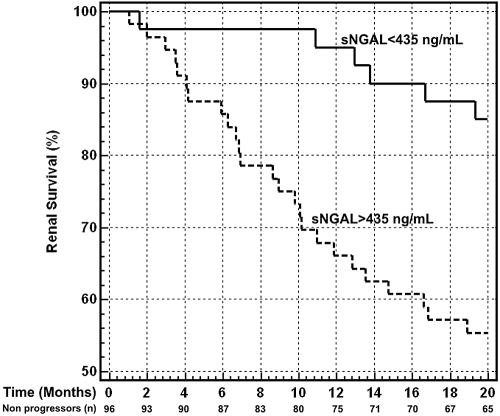
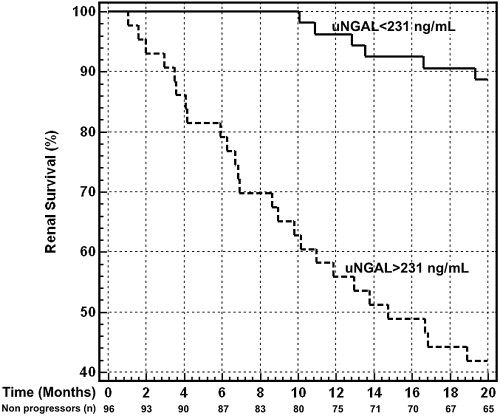
Results: At baseline, both serum and urinary NGAL were inversely, independently, and closely related to eGFR. After a median follow-up of 18.5 mo (range 1.01 to 20), 31 patients (32%) reached the composite endpoint. At baseline, these patients were significantly older and showed increased serum creatinine, calcium-phosphate product, C-reactive protein, fibrinogen, daily proteinuria, and NGAL levels, whereas eGFR values were significantly lower. Univariate followed by multivariate Cox proportional hazard regression analysis showed that urinary NGAL and sNGAL predicted CKD progression independently of other potential confounders, including eGFR and age.
Conclusion: In patients with CKD, NGAL closely reflects the entity of renal impairment and represents a strong and independent risk marker for progression of CKD.
Figures

References
-
- Kent DM, Jafar TH, Hayward RA, Tighiouart H, Landa M, de Jong P, de Zeeuw D, Remuzzi G, Kamper AL, Levey AS: Progression risk, urinary protein excretion, and treatment effects of angiotensin-converting enzyme inhibitors in nondiabetic kidney disease. J Am Soc Nephrol 18: 1959–1965, 2007 - PubMed
-
- Hunsicker LG, Adler S, Caggiula A, England BK, Greene T, Kusek JW, Rogers NL, Teschan PE: Predictors of the progression of renal disease in the Modification of Diet in Renal Disease Study. Kidney Int 51: 1908–1919, 1997 - PubMed
-
- Eddy AA, Neilson EG. Chronic kidney disease progression: J Am Soc Nephrol 17: 2964–2966, 2006 - PubMed
-
- Phillips AO: The role of renal proximal tubular cells in diabetic nephropathy. Curr Diab Rep 3: 491–496, 2003 - PubMed
-
- Bruzzi I, Remuzzi G, Benigni A: Endothelin: A mediator of renal disease progression. J Nephrol 10: 179–183, 1997 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
