

Addition of adult-to-adult living donation to liver transplant programs improves survival but at an increased cost
- PMID: 19177435
- PMCID: PMC3222562
- DOI: 10.1002/lt.21671
Addition of adult-to-adult living donation to liver transplant programs improves survival but at an increased cost
Abstract
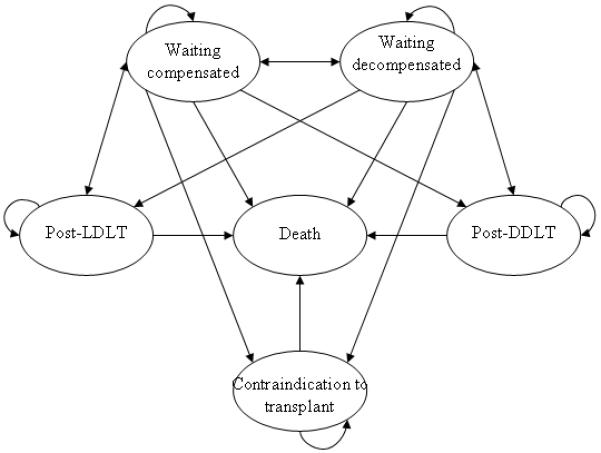
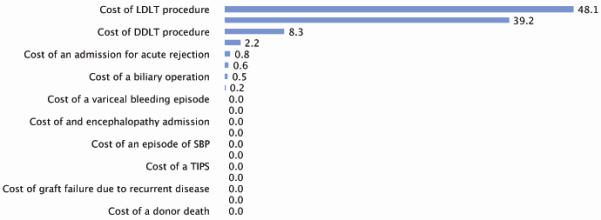
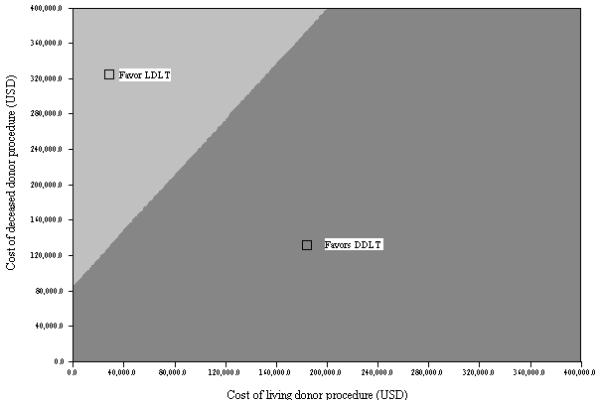
Using outcomes data from the Adult-to-Adult Living Donor Liver Transplantation Cohort Study, we performed a cost-effectiveness analysis exploring the costs and benefits of living donor liver transplantation (LDLT). A multistage Markov decision analysis model was developed with treatment, including medical management only (strategy 1), waiting list with possible deceased donor liver transplantation (DDLT; strategy 2), and waiting list with possible LDLT or DDLT (strategy 3) over 10 years. Decompensated cirrhosis with medical management offered survival of 2.0 quality-adjusted life years (QALYs) while costing an average of $65,068, waiting list with possible DDLT offered 4.4-QALY survival and a mean cost of $151,613, and waiting list with possible DDLT or LDLT offered 4.9-QALY survival and a mean cost of $208,149. Strategy 2 had an incremental cost-effectiveness ratio (ICER) of $35,976 over strategy 1, whereas strategy 3 produced an ICER of $106,788 over strategy 2. On average, strategy 3 cost $47,693 more per QALY than strategy 1. Both DDLT and LDLT were cost-effective compared to medical management of cirrhosis over our 10-year study period. The addition of LDLT to a standard waiting list DDLT program is effective at improving recipient survival and preventing waiting list deaths but at a greater cost.
(c) 2009 AASLD.
Figures

Similar articles
-
Evaluation of the Intention-to-Treat Benefit of Living Donation in Patients With Hepatocellular Carcinoma Awaiting a Liver Transplant.JAMA Surg. 2021 Sep 1;156(9):e213112. doi: 10.1001/jamasurg.2021.3112. Epub 2021 Sep 8. JAMA Surg. 2021. PMID: 34259797 Free PMC article.
-
Waiting list mortality for pediatric deceased donor liver transplantation in a Japanese living-donor-dominant program.Pediatr Transplant. 2019 Dec;23(8):e13578. doi: 10.1111/petr.13578. Epub 2019 Sep 19. Pediatr Transplant. 2019. PMID: 31535772
-
Liver transplant recipient survival benefit with living donation in the model for endstage liver disease allocation era.Hepatology. 2011 Oct;54(4):1313-21. doi: 10.1002/hep.24494. Hepatology. 2011. PMID: 21688284 Free PMC article.
-
Does living donation have advantages over deceased donation in liver transplantation?J Gastroenterol Hepatol. 2010 Oct;25(10):1598-603. doi: 10.1111/j.1440-1746.2010.06418.x. J Gastroenterol Hepatol. 2010. PMID: 20880167 Review.
-
Living donor liver transplantation.Curr Opin Organ Transplant. 2010 Jun;15(3):283-7. doi: 10.1097/MOT.0b013e32833983ee. Curr Opin Organ Transplant. 2010. PMID: 20489627 Review.
Cited by
-
Comparative effectiveness of donation after cardiac death versus donation after brain death liver transplantation: Recognizing who can benefit.Liver Transpl. 2012 Jun;18(6):630-40. doi: 10.1002/lt.23418. Liver Transpl. 2012. PMID: 22645057 Free PMC article.
-
Predicting Liver Transplant Capacity Using Discrete Event Simulation.Med Decis Making. 2015 Aug;35(6):784-96. doi: 10.1177/0272989X14559055. Epub 2014 Nov 12. Med Decis Making. 2015. PMID: 25391681 Free PMC article.
-
Role of liver transplantation for hepatocellular carcinoma.J Clin Exp Hepatol. 2014 Aug;4(Suppl 3):S97-S103. doi: 10.1016/j.jceh.2014.01.002. Epub 2014 Jan 23. J Clin Exp Hepatol. 2014. PMID: 25755618 Free PMC article. Review.
-
Role of living donor liver transplantation in the treatment of hepatitis C virus infection.Hepat Mon. 2011 Jun;11(6):427-33. Hepat Mon. 2011. PMID: 22087173 Free PMC article.
-
Optimal Endoscopic Management of Anastomotic Strictures After Double- Biliary Reconstruction in Right Lobe Living-Donor Liver Transplantation.Balkan Med J. 2021 Nov;38(6):348-356. doi: 10.5152/balkanmedj.2021.21692. Balkan Med J. 2021. PMID: 34860162 Free PMC article.
References
-
- Hashikura Y, Kawasaki S, Terada M, Ikegami T, Nakazawa Y, Urata K, et al. Long-term results of living-related donor liver graft transplantation: a single-center analysis of 110 transplants. Transplantation. 2001;72(1):95–99. - PubMed
-
- Fujita S, Kim ID, Uryuhara K, Asonuma K, Egawa H, Kiuchi T, et al. Hepatic grafts from live donors: donor morbidity for 470 cases of live donation. Transplant International. 2000;13(5):333–339. - PubMed
-
- Ghobrial R, Freise C, Trotter J, Tong L, Ojo A, Fair J, et al. Donor morbidity and mortality of adult living donors for liver transplantation (abstract) Am J Transpl. 2006;6(S2):115.
-
- Bonsel GJ, Klompmaker IJ, Essink-Bot ML, Habbema JD, Slooff MJ. Cost-effectiveness analysis of the Dutch liver transplantation programme. Transplantation Proceedings. 1990;22(4):1481–1484. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK062496/DK/NIDDK NIH HHS/United States
- P30 DK067629/DK/NIDDK NIH HHS/United States
- U01 DK062536/DK/NIDDK NIH HHS/United States
- U01-DK62444/DK/NIDDK NIH HHS/United States
- U01-DK62536/DK/NIDDK NIH HHS/United States
- U01-DK62505/DK/NIDDK NIH HHS/United States
- U01 DK062498/DK/NIDDK NIH HHS/United States
- U01 DK062484/DK/NIDDK NIH HHS/United States
- U01-DK62483/DK/NIDDK NIH HHS/United States
- U01 DK062483/DK/NIDDK NIH HHS/United States
- U01 DK062467/DK/NIDDK NIH HHS/United States
- U01-DK62467/DK/NIDDK NIH HHS/United States
- U01 DK062531/DK/NIDDK NIH HHS/United States
- U01 DK062444/DK/NIDDK NIH HHS/United States
- U01-DK62531/DK/NIDDK NIH HHS/United States
- U01-DK62484/DK/NIDDK NIH HHS/United States
- U01 DK062505/DK/NIDDK NIH HHS/United States
- U01-DK62494/DK/NIDDK NIH HHS/United States
- U01-DK62498/DK/NIDDK NIH HHS/United States
- U01-DK62496/DK/NIDDK NIH HHS/United States
- U01 DK062494/DK/NIDDK NIH HHS/United States