

Cardiovascular therapies and associated glucose homeostasis: implications across the dysglycemia continuum
- PMID: 19179214
- PMCID: PMC2655143
- DOI: 10.1016/j.jacc.2008.10.037
Cardiovascular therapies and associated glucose homeostasis: implications across the dysglycemia continuum
Abstract
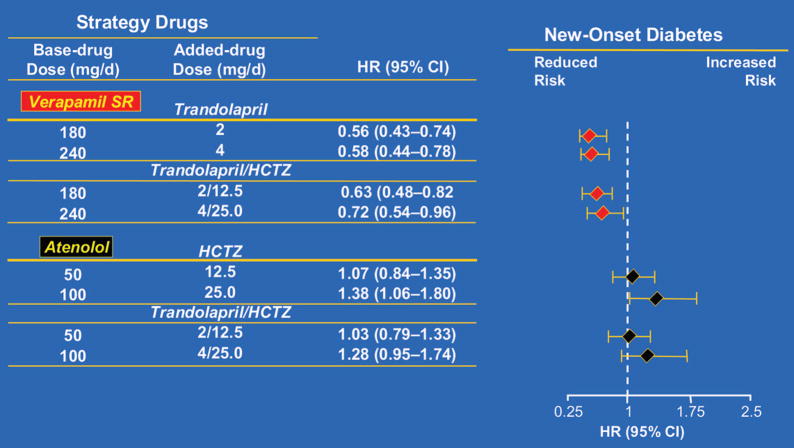
Certain cardiovascular drugs have adverse effects on glucose homeostasis, which may lead to important long-term implications for increased risks of adverse outcomes. Thiazide diuretics, niacin, and beta-adrenergic blockers impair glucose homeostasis. However, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers have demonstrated beneficial metabolic effects. The newer vasodilating beta-blocking agents and calcium antagonists appear to be metabolically neutral. These considerations, in addition to meticulous attention to blood pressure control and lifestyle changes, have the potential to beneficially modify glycemia and long-term risks. These considerations have particular importance in younger patients who may also have pre-diabetes or the metabolic syndrome and who are likely to require therapy over the course of decades.
Conflict of interest statement
Figures

Similar articles
-
Add-On Antihypertensive Medications to Angiotensin-Aldosterone System Blockers in Diabetes: A Comparative Effectiveness Study.Clin J Am Soc Nephrol. 2018 May 7;13(5):727-734. doi: 10.2215/CJN.09510817. Epub 2018 Mar 23. Clin J Am Soc Nephrol. 2018. PMID: 29572286 Free PMC article.
-
A review of chemical therapies for treating diabetic hypertension.Expert Opin Pharmacother. 2017 Jun;18(9):909-923. doi: 10.1080/14656566.2017.1328054. Epub 2017 May 16. Expert Opin Pharmacother. 2017. PMID: 28480805 Review.
-
The metabolic syndrome in hypertension: European society of hypertension position statement.J Hypertens. 2008 Oct;26(10):1891-900. doi: 10.1097/HJH.0b013e328302ca38. J Hypertens. 2008. PMID: 18806611
-
Antihypertensive medications and blood sugar: theories and implications.Can J Cardiol. 2006 Mar 1;22(3):229-33. doi: 10.1016/s0828-282x(06)70902-3. Can J Cardiol. 2006. PMID: 16520854 Free PMC article. Review.
-
The effects of antihypertensive drugs on glucose metabolism.Diabetes Obes Metab. 2024 Nov;26(11):4820-4829. doi: 10.1111/dom.15821. Epub 2024 Aug 14. Diabetes Obes Metab. 2024. PMID: 39140233 Review.
Cited by
-
12S-hydroxyeicosatetraenoic acid levels link to coronary artery disease in Type 2 diabetic patients.J Endocrinol Invest. 2013 Jun;36(6):385-9. doi: 10.3275/8654. Epub 2012 Oct 22. J Endocrinol Invest. 2013. PMID: 23095287
-
Impact of chronic diuretic treatment on glucose homeostasis.Diabetol Metab Syndr. 2013 Dec 13;5(1):80. doi: 10.1186/1758-5996-5-80. Diabetol Metab Syndr. 2013. PMID: 24330854 Free PMC article.
-
Lymphocyte to High-Density Lipoprotein Ratio but Not Platelet to Lymphocyte Ratio Effectively Predicts Metabolic Syndrome Among Subjects From Rural China.Front Cardiovasc Med. 2021 Mar 12;8:583320. doi: 10.3389/fcvm.2021.583320. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33778016 Free PMC article.
-
Metabolic hypertension: concept and practice.Front Med. 2013 Jun;7(2):201-6. doi: 10.1007/s11684-013-0264-4. Epub 2013 Apr 5. Front Med. 2013. PMID: 23564405 Review.
-
Antihypertensive medications: benefits of blood pressure lowering and hazards of metabolic effects.Expert Rev Cardiovasc Ther. 2009 Jun;7(6):689-702. doi: 10.1586/erc.09.31. Expert Rev Cardiovasc Ther. 2009. PMID: 19505284 Free PMC article. Review.
References
-
- American Diabetes Association [online] [Accessed August 21, 2008]. Available at: http://www.diabetes.org/advocacy-and-legalresources/cost-of-diabetes.jsp.
-
- American Heart Association. Heart Disease and Stroke Statistics 2008 Update [online] [Accessed August 21, 2008]. Available at: http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.107.187998.
-
- Bakris GL, Gaxiola E, Messerli FH, et al. Clinical outcomes in the diabetes cohort of the INternational VErapamil SR-Trandolapril study. Hypertension. 2004;44:637–42. - PubMed
-
- Whiteley L, Padmanabhan S, Hole D, Isles C. Should diabetes be considered a coronary heart disease risk equivalent?: results from 25 years of follow-up in the Renfrew and Paisley survey. Diabetes Care. 2005;28:1588–93. - PubMed
-
- Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA. 2003;290:1884–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
