

Staphylococcus aureus bacteraemia in a tropical setting: patient outcome and impact of antibiotic resistance
- PMID: 19180198
- PMCID: PMC2628727
- DOI: 10.1371/journal.pone.0004308
Staphylococcus aureus bacteraemia in a tropical setting: patient outcome and impact of antibiotic resistance
Abstract
Background: Most information on invasive Staphylococcus aureus infections comes from temperate countries. There are considerable knowledge gaps in epidemiology, treatment, drug resistance and outcome of invasive S. aureus infection in the tropics.
Methods: A prospective, observational study of S. aureus bacteraemia was conducted in a 1000-bed regional hospital in northeast Thailand over 1 year. Detailed clinical data were collected and final outcomes determined at 12 weeks, and correlated with antimicrobial susceptibility profiles of infecting isolates.
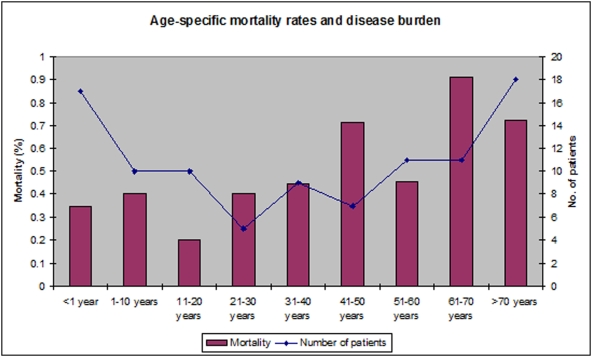
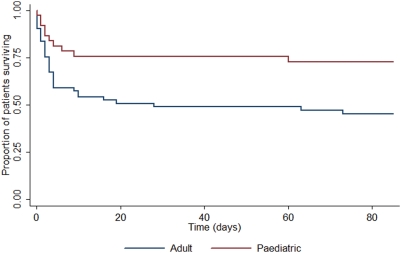
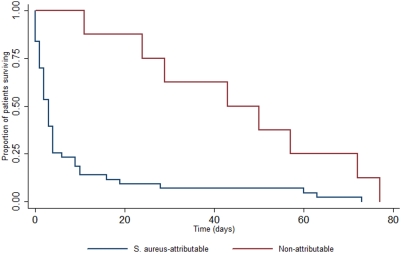
Principal findings: Ninety-eight patients with S. aureus bacteraemia were recruited. The range of clinical manifestations was similar to that reported from temperate countries. The prevalence of endocarditis was 14%. The disease burden was highest at both extremes of age, whilst mortality increased with age. The all-cause mortality rate was 52%, with a mortality attributable to S. aureus of 44%. Methicillin-resistant S. aureus (MRSA) was responsible for 28% of infections, all of which were healthcare-associated. Mortality rates for MRSA and methicillin-susceptible S. aureus (MSSA) were 67% (18/27) and 46% (33/71), respectively (p = 0.11). MRSA isolates were multidrug resistant. Only vancomycin or fusidic acid would be suitable as empirical treatment options for suspected MRSA infection.
Conclusions: S. aureus is a significant pathogen in northeast Thailand, with comparable clinical manifestations and a similar endocarditis prevalence but higher mortality than industrialised countries. S. aureus bacteraemia is frequently associated with exposure to healthcare settings with MRSA causing a considerable burden of disease. Further studies are required to define setting-specific strategies to reduce mortality from S. aureus bacteraemia, prevent MRSA transmission, and to define the burden of S. aureus disease and emergence of drug resistance throughout the developing world.
Conflict of interest statement
Figures
References
-
- Lowy FD. Staphylococcus aureus infections. N Engl J Med. 1998;339:520–532. - PubMed
-
- Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, et al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39:309–317. - PubMed
-
- Wallin TR, Hern HG, Frazee BW. Community-associated methicillin-resistant Staphylococcus aureus. Emerg Med Clin North Am. 2008;26:431–455, ix. - PubMed
-
- Powell JP, Wenzel RP. Antibiotic options for treating community-acquired MRSA. Expert Rev Anti Infect Ther. 2008;6:299–307. - PubMed
-
- Hill PC, Birch M, Chambers S, Drinkovic D, Ellis-Pegler RB, et al. Prospective study of 424 cases of Staphylococcus aureus bacteraemia: determination of factors affecting incidence and mortality. Intern Med J. 2001;31:97–103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
