

Molecular framework for response to imatinib mesylate in systemic sclerosis
- PMID: 19180499
- PMCID: PMC2638060
- DOI: 10.1002/art.24221
Molecular framework for response to imatinib mesylate in systemic sclerosis
Abstract
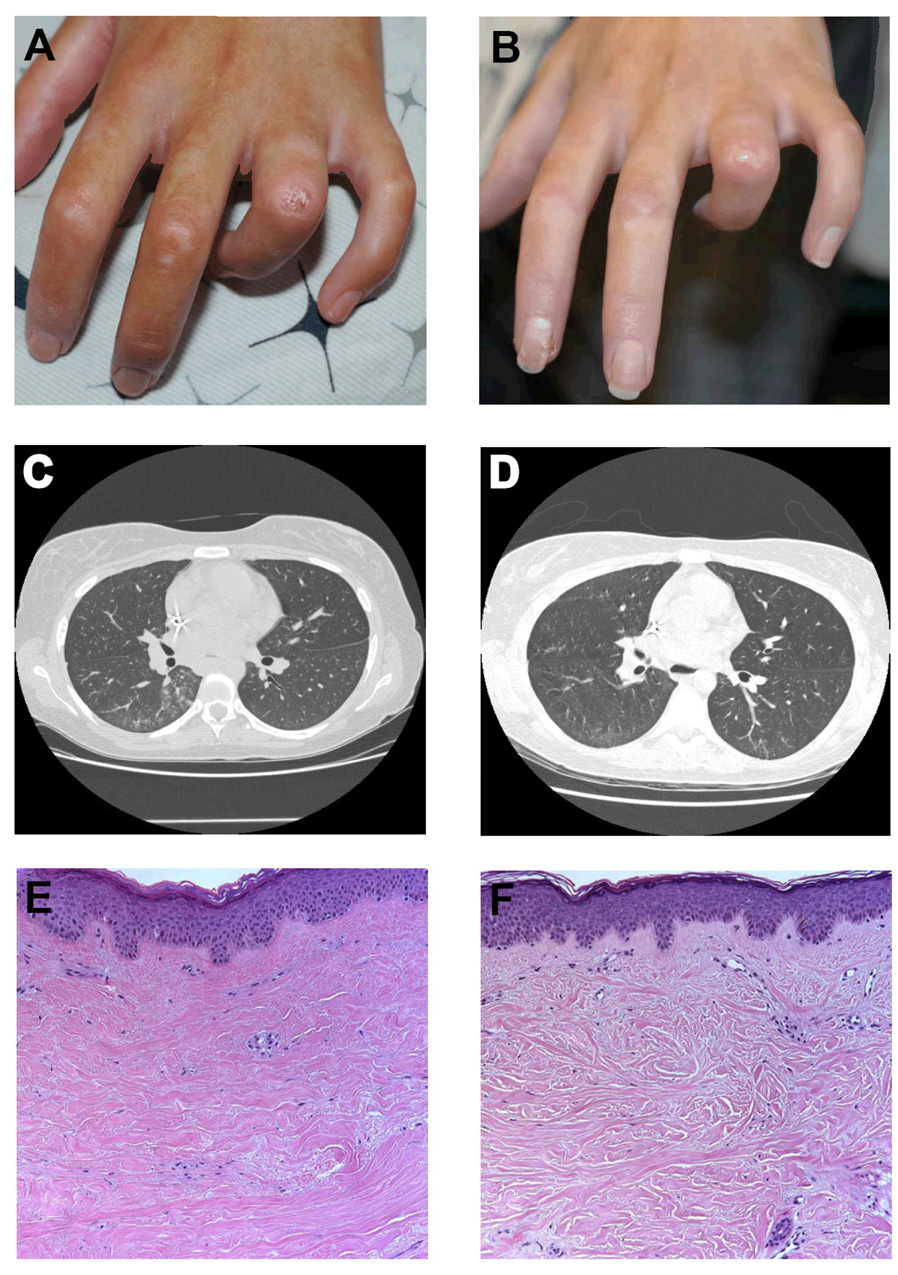
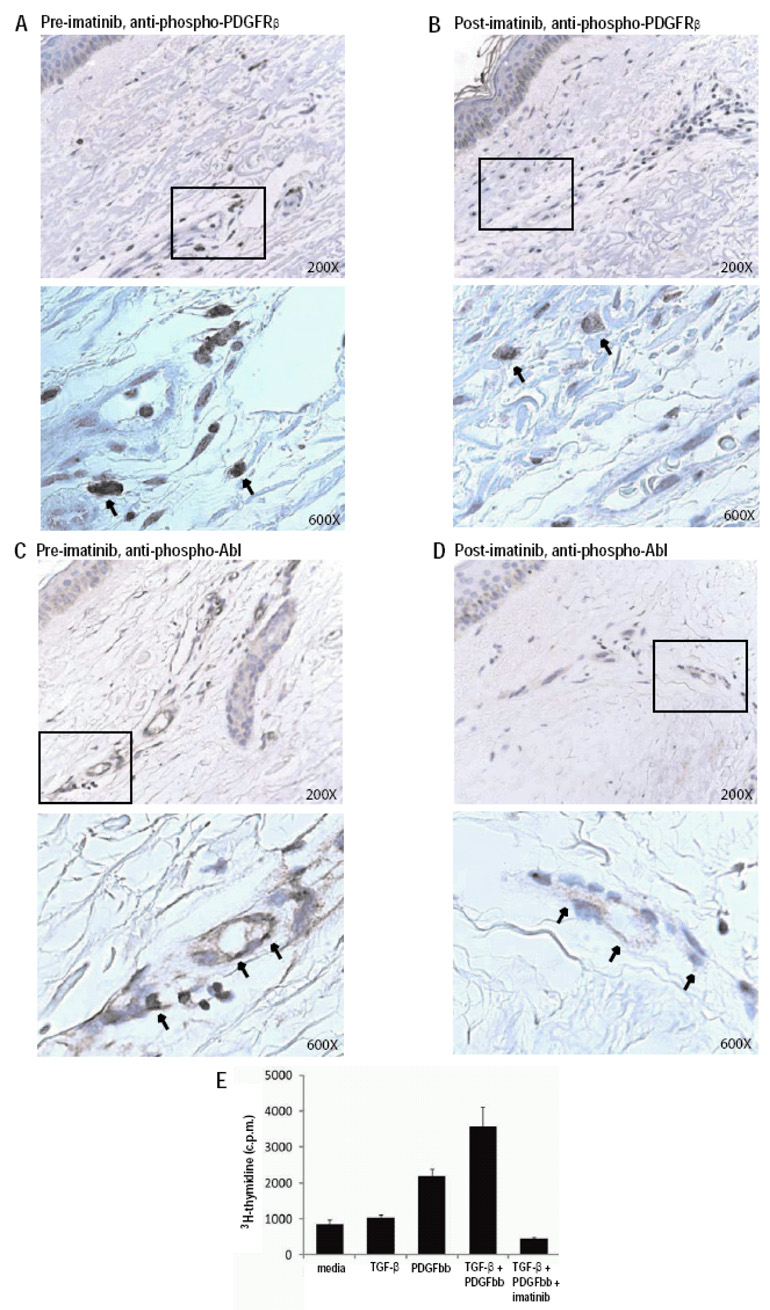
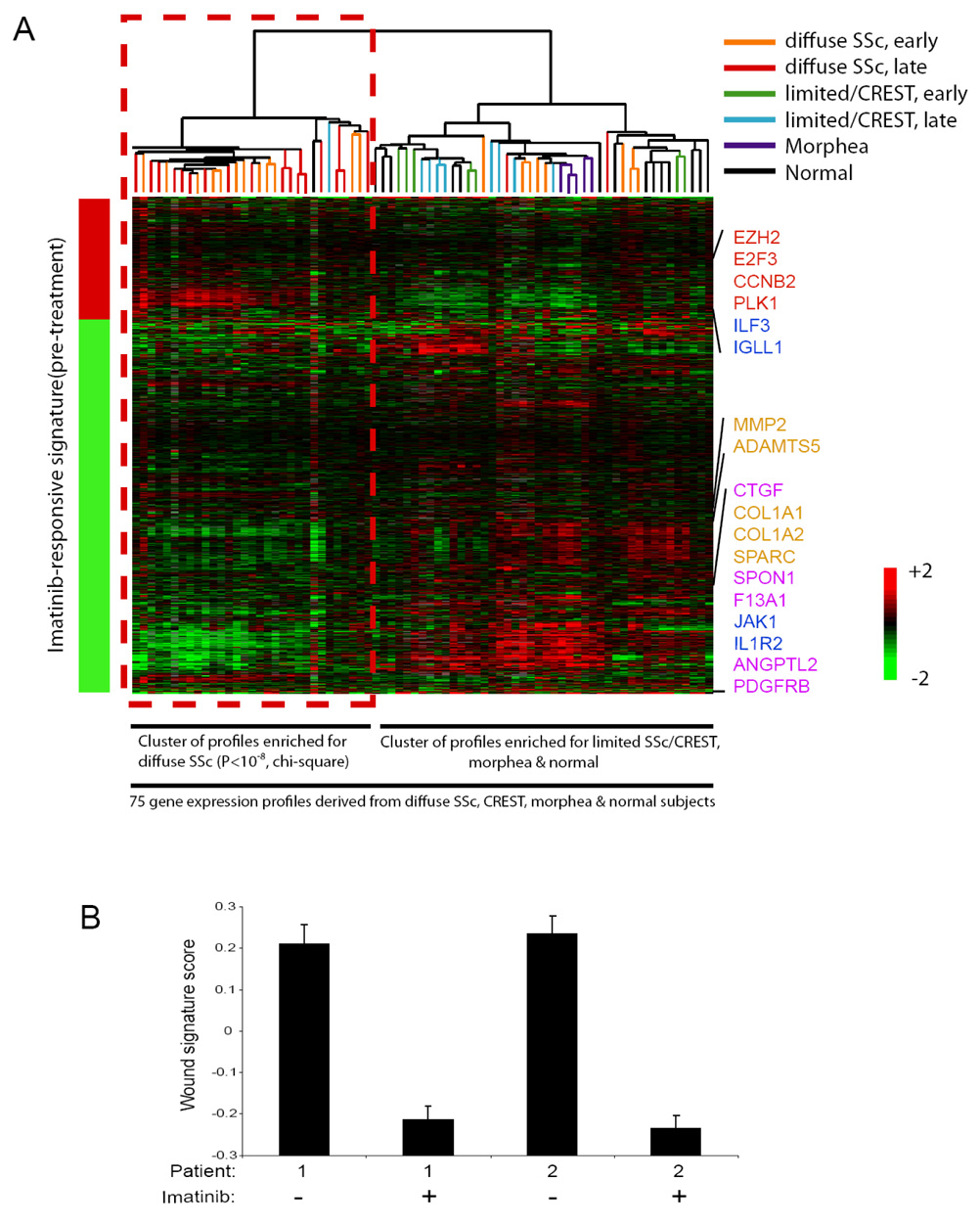
Systemic sclerosis (SSc) is an autoimmune disease in which the tyrosine kinases platelet-derived growth factor receptor (PDGFR) and Abl are hypothesized to contribute to the fibrosis and vasculopathy of the skin and internal organs. Herein we describe 2 patients with early diffuse cutaneous SSc (dcSSc) who experienced reductions in cutaneous sclerosis in response to therapy with the tyrosine kinase inhibitor imatinib mesylate. Immunohistochemical analyses of skin biopsy specimens demonstrated reductions of phosphorylated PDGFRbeta and Abl with imatinib therapy. By gene expression profiling, an imatinib-responsive signature specific to dcSSc was identified (P < 10(-8)). The response of these patients and the findings of the analyses suggest that PDGFRbeta and Abl play critical, synergistic roles in the pathogenesis of SSc, and that imatinib targets a gene expression program that is frequently dysregulated in dcSSc.
Figures
References
-
- Baroni SS, Santillo M, Bevilacqua F, Luchetti M, Spadoni T, Mancini M, et al. Stimulatory autoantibodies to the PDGF receptor in systemic sclerosis. N Engl J Med. 2006;354(25):2667–2676. - PubMed
-
- Ludwicka A, Ohba T, Trojanowska M, Yamakage A, Strange C, Smith EA, et al. Elevated levels of platelet derived growth factor and transforming growth factor-beta 1 in bronchoalveolar lavage fluid from patients with scleroderma. J Rheumatol. 1995;22(10):1876–1883. - PubMed
-
- Soria A, Cario-Andre M, Lepreux S, Rezvani HR, Pasquet JM, Pain C, et al. The effect of imatinib (Glivec) on scleroderma and normal dermal fibroblasts: a preclinical study. Dermatology. 2008;216(2):109–117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
