

Treatment of selective serotonin reuptake inhibitor-resistant depression in adolescents: predictors and moderators of treatment response
- PMID: 19182688
- PMCID: PMC2754157
- DOI: 10.1097/chi.0b013e3181977476
Treatment of selective serotonin reuptake inhibitor-resistant depression in adolescents: predictors and moderators of treatment response
Abstract
Objective: To advance knowledge regarding strategies for treating selective serotonin reuptake inhibitor (SSRI)-resistant depression in adolescents, we conducted a randomized controlled trial evaluating alternative treatment strategies. In primary analyses, cognitive-behavioral therapy (CBT) combined with medication change was associated with higher rates of positive response to short-term (12-week) treatment than medication alone. This study examines predictors and moderators of treatment response, with the goal of informing efforts to match youths to optimal treatment strategies.
Method: Youths who had not improved during an adequate SSRI trial (N = 334) were randomized to an alternative SSRI, an alternative SSRI plus CBT, venlafaxine, or venlafaxine plus CBT. Analyses examined predictors and moderators of treatment response.
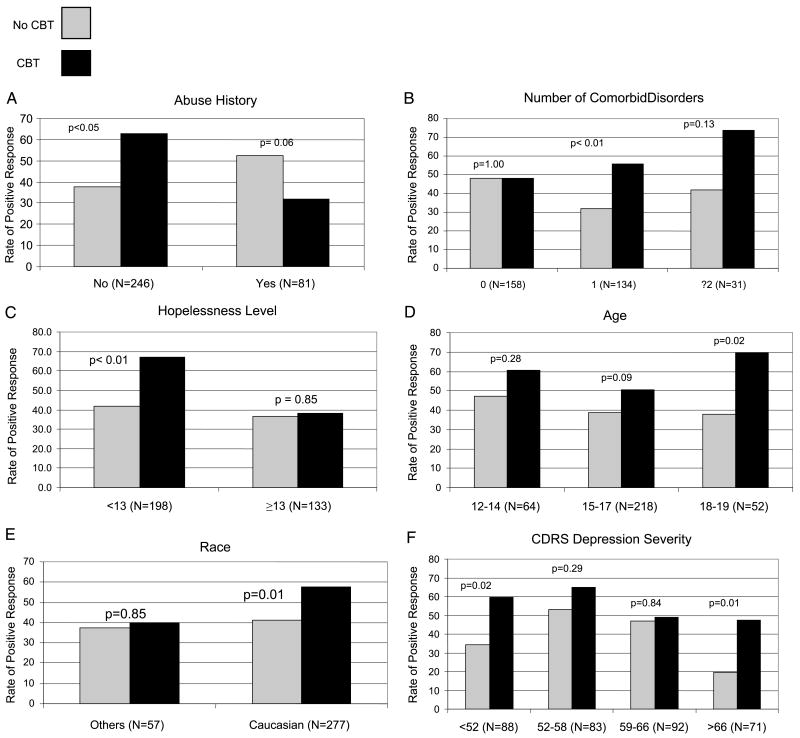
Results: Less severe depression, less family conflict, and absence of nonsuicidal self-injurious behavior predicted better treatment response status. Significant moderators of response to CBT + medication (combined) treatment were number of comorbid disorders and abuse history; hopelessness was marginally significant. The CBT/combined treatment superiority over medication alone was more evident among youths who had more comorbid disorders (particularly attention-deficit/hyperactivity disorder and anxiety disorders), no abuse history, and lower hopelessness. Further analyses revealed a stronger effect of combined CBT + medication treatment among youths who were older and white and had no nonsuicidal self-injurious behavior and longer prestudy pharmacotherapy.
Conclusions: Combined treatment with CBT and antidepressant medication may be more advantageous for adolescents whose depression is comorbid with other disorders. Given the additional costs of adding CBT to medication, consideration of moderators in clinical decision making can contribute to a more personalized and effective approach to treatment.
Conflict of interest statement
Disclosure: Dr. Asarnow consults on cognitive-behavioral therapy and cognitive-behavioral therapy for depression, previously consulted on an unrestricted grant from Pfizer, and receives unrestricted research funding from Philip Morris; a family member receives funding from Bristol-Myers Squibb. Dr. Birmaher has participated in forums sponsored by Solvay Pharmaceuticals and Abcomm. He has presented on bipolar disorders in children at a meeting sponsored by Solvay. Dr. Birmaher has also received royalties from Random House, has participated in regional advisory board meetings for Jazz, and has provided training on the K-SADS-PL rating scale to Shire. Dr. Emslie receives research support from NIMH, Shire, Somerset, Forest Laboratories, and Biobehavioral Diagnostics; is a consultant to Eli Lilly, Forest, Pfizer, Validus Pharmaceuticals, Wyeth-Ayerst, Shire, and Biobehavioral Diagnostics. The other authors report no conflicts of interest.
Figures
Comment in
-
In adolescents with SSRI resistant depression, CBT/combined treatment is most effective in those with comorbid disorders.Evid Based Ment Health. 2009 Nov;12(4):108. doi: 10.1136/ebmh.12.4.108. Evid Based Ment Health. 2009. PMID: 19854770 No abstract available.
References
-
- Birmaher B, Brent D. Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. [March 10, 2008]. http://www.aacap.org/galleries/PracticeParameters/InPress_2007_Depressiv.... - PubMed
-
- Domino ME, Burns BJ, Silva SG, et al. Cost-effectiveness of treatments for adolescent depression: results from TADS. Am J Psychiatry. 2008;165:588–596. - PubMed
-
- Kraemer HC, Wilson GT, Fairburn CG, Agras WS. Mediators and moderators of treatment effects in randomized clinical trials. Arch Gen Psychiatry. 2002;59:877–883. - PubMed
-
- Curry J, Rohde P, Simons A, et al. Predictors and moderators of acute outcome in the Treatment for Adolescents with Depression Study (TADS) J Am Acad Child Adolesc Psychiatry. 2006;45:1427–1439. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 MH061835/MH/NIMH NIH HHS/United States
- MH61835/MH/NIMH NIH HHS/United States
- U01 MH061958/MH/NIMH NIH HHS/United States
- U01 MH061864/MH/NIMH NIH HHS/United States
- MH66371/MH/NIMH NIH HHS/United States
- MH61869/MH/NIMH NIH HHS/United States
- U01 MH061869/MH/NIMH NIH HHS/United States
- U01 MH061856/MH/NIMH NIH HHS/United States
- U01 MH062014/MH/NIMH NIH HHS/United States
- MH62014/MH/NIMH NIH HHS/United States
- MH61958/MH/NIMH NIH HHS/United States
- MH61864/MH/NIMH NIH HHS/United States
- P30 MH066371/MH/NIMH NIH HHS/United States
- MH61856/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
