

Effects of study design and trends for EVAR versus OSR
- PMID: 19183749
- PMCID: PMC2605334
- DOI: 10.2147/vhrm.s3810
Effects of study design and trends for EVAR versus OSR
Abstract
Purpose: To investigate if study design factors such as randomization, multi-center versus single center evidence, institutional surgical volume, and patient selection affect the outcomes for endovascular repair (EVAR) versus open surgical repair (OSR). Finally, we investigate trends over time in EVAR versus OSR outcomes.
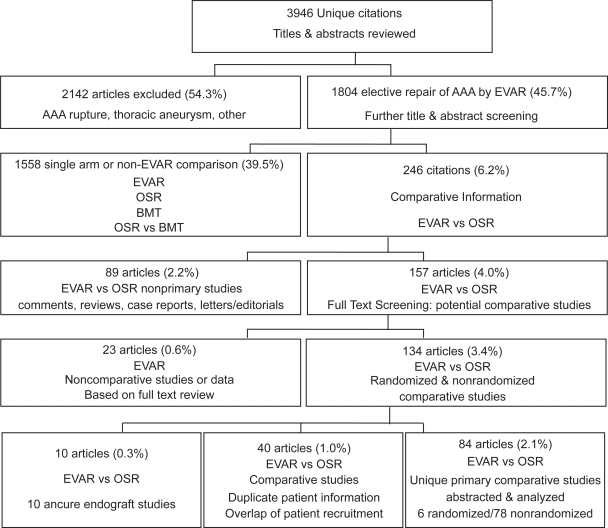
Methods: Search strategies for comparative studies were performed individually for: OVID's MEDLINE, EMBASE, CINAHL, HAPI, and Evidence Based Medicine (EBM) Reviews (including Cochrane DSR, ACP Journal Club, DARE and CCTR), limited to 1990 and November 2006.
Results: Identified literature: 84 comparative studies pertaining to 57,645 patients. These include 4 randomized controlled trials (RCTs), plus 2 RCTs with long-term follow-up. The other 78 comparative studies were nonrandomized with 75 reporting perioperative outcomes, of which 16 were multi-center, and 59 single-center studies. Of the single-center studies 31 were low-volume and 28 were high-volume centers. In addition, 5 studies had all patients anatomically eligible for EVAR, and 8 studies included high-risk patients only. Finally, 25 long term observational studies reported outcomes up to 3 years.
Outcomes: Lower perioperative mortality and rates of complications for EVAR versus OSR varied across study designs and patient populations. EVAR adverse outcomes have decreased in recent times.
Conclusion: EVAR highlights the problem of performing meta-analysis when the experience evolves over time.
Keywords: abdominal aortic aneurysm; endovascular repair; meta-analysis; open surgical repair; systematic review.
Similar articles
-
Laparoscopic surgery for elective abdominal aortic aneurysm repair.Cochrane Database Syst Rev. 2017 May 4;5(5):CD012302. doi: 10.1002/14651858.CD012302.pub2. Cochrane Database Syst Rev. 2017. PMID: 28471523 Free PMC article.
-
Endovascular treatment for ruptured abdominal aortic aneurysm.Cochrane Database Syst Rev. 2017 May 26;5(5):CD005261. doi: 10.1002/14651858.CD005261.pub4. Cochrane Database Syst Rev. 2017. PMID: 28548204 Free PMC article.
-
Hospital Volume and Social Determinants of Health Do Not Impact Outcomes in Fenestrated Visceral Segment Endovascular Aortic Repair for Patients Treated at VQI Centers.Vasc Endovascular Surg. 2025 Aug;59(6):584-593. doi: 10.1177/15385744251330017. Epub 2025 Mar 24. Vasc Endovascular Surg. 2025. PMID: 40127376
-
A systematic review and meta-analysis evaluating the impact of obesity on outcomes of abdominal aortic aneurysm treatment.J Vasc Surg. 2022 Apr;75(4):1450-1455.e3. doi: 10.1016/j.jvs.2021.10.053. Epub 2021 Nov 14. J Vasc Surg. 2022. PMID: 34785300
-
Editor's Choice - The Implications of Non-compliance to Endovascular Aneurysm Repair Surveillance: A Systematic Review and Meta-analysis.Eur J Vasc Endovasc Surg. 2018 Apr;55(4):492-502. doi: 10.1016/j.ejvs.2017.11.030. Epub 2018 Jan 5. Eur J Vasc Endovasc Surg. 2018. PMID: 29307756 Free PMC article.
Cited by
-
Ten-year results of endovascular abdominal aortic aneurysm repair from a large multicenter registry.J Vasc Surg. 2013 Aug;58(2):324-32. doi: 10.1016/j.jvs.2013.01.051. Epub 2013 May 14. J Vasc Surg. 2013. PMID: 23683376 Free PMC article.
-
Should endovascular repair be reimbursed for low risk abdominal aortic aneurysm patients? Evidence from ontario, Canada.Int J Vasc Med. 2011;2011:308685. doi: 10.1155/2011/308685. Epub 2011 Jun 24. Int J Vasc Med. 2011. PMID: 21748018 Free PMC article.
-
Bayesian hierarchical models combining different study types and adjusting for covariate imbalances: a simulation study to assess model performance.PLoS One. 2011;6(10):e25635. doi: 10.1371/journal.pone.0025635. Epub 2011 Oct 10. PLoS One. 2011. PMID: 22016772 Free PMC article.
-
The importance of adjusting for potential confounders in Bayesian hierarchical models synthesising evidence from randomised and non-randomised studies: an application comparing treatments for abdominal aortic aneurysms.BMC Med Res Methodol. 2010 Jul 9;10:64. doi: 10.1186/1471-2288-10-64. BMC Med Res Methodol. 2010. PMID: 20618973 Free PMC article.
References
-
- Aarts F, van Sterkenburg S, Blankensteijn JD. Endovascular aneurysm repair versus open aneurysm repair: comparison of treatment outcome and procedure-related reintervention rate. Ann Vasc Surg. 2005;19:699–704. - PubMed
-
- Aho PS, Niemi T, Lindgren L, et al. Endovascular vs open AAA repair: Similar effects on renal proximal tubular function. Scand J Surg. 2004;93:52–6. - PubMed
-
- Akkersdijk GJM, Prinssen M, Blankensteijn JD. The impact of endovascular treatment on in-hospital mortality following non-ruptured AAA repair over a decade: A population based study of 16,446 patients. Eur J Vasc Endovasc Surg. 2004;28:41–6. - PubMed
-
- Anderson PL, Arons RR, Moskowitz AJ, et al. A statewide experience with endovascular abdominal aortic aneurysm repair: Rapid diffusion with excellent early results. J Vasc Surg. 2004;39:10–9. - PubMed
-
- Angle N, Dorafshar AH, Moore WS, et al. Open versus endovascular repair of abdominal aortic aneurysms: What does each really cost? Ann Vasc Surg. 2004;18:612–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
