

Arterial pulmonary hypertension in noncardiac intensive care unit
- PMID: 19183752
- PMCID: PMC2605326
- DOI: 10.2147/vhrm.s3998
Arterial pulmonary hypertension in noncardiac intensive care unit
Abstract
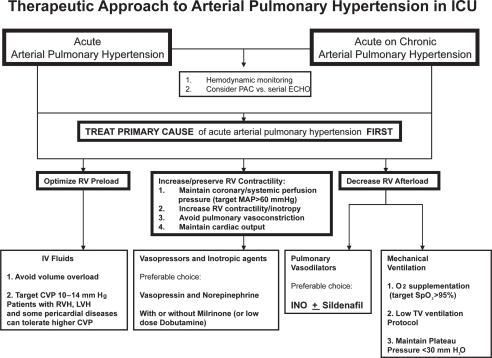
Pulmonary artery pressure elevation complicates the course of many complex disorders treated in a noncardiac intensive care unit. Acute pulmonary hypertension, however, remains underdiagnosed and its treatment frequently begins only after serious complications have developed. Significant pathophysiologic differences between acute and chronic pulmonary hypertension make current classification and treatment recommendations for chronic pulmonary hypertension barely applicable to acute pulmonary hypertension. In order to clarify the terminology of acute pulmonary hypertension and distinguish it from chronic pulmonary hypertension, we provide a classification of acute pulmonary hypertension according to underlying pathophysiologic mechanisms, clinical features, natural history, and response to treatment. Based on available data, therapy of acute arterial pulmonary hypertension should generally be aimed at acutely relieving right ventricular (RV) pressure overload and preventing RV dysfunction. Cases of severe acute pulmonary hypertension complicated by RV failure and systemic arterial hypotension are real clinical challenges requiring tight hemodynamic monitoring and aggressive treatment including combinations of pulmonary vasodilators, inotropic agents and systemic arterial vasoconstrictors. The choice of vasopressor and inotropes in patients with acute pulmonary hypertension should take into consideration their effects on vascular resistance and cardiac output when used alone or in combinations with other agents, and must be individualized based on patient response.
Keywords: acute cor pulmonale; acute pulmonary hypertension; cor pulmonale; pulmonary hypertension; right heart failure.
Figures
References
-
- Adrie C, Holzmann A, Hirani WM, et al. Effects of intravenous Zaprinast and inhaled nitric oxide on pulmonary hemodynamics and gas exchange in an ovine model of acute respiratory distress syndrome. Anesthesiology. 2000;93:422–30. - PubMed
-
- Albertini M, Ciminaghi B, Mazzola S, et al. Improvement of respiratory function by bosentan during endotoxic shock in the pig. Prostaglandins Leukot Essent Fatty Acids. 2001;65:103–8. - PubMed
-
- Arafa OE, Geiran OR, Andersen K, et al. Intraaortic balloon pumping for predominantly right ventricular failure after heart transplantation. Ann Thorac Surg. 2000;70:1587–93. - PubMed
-
- Atz AM, Wessel DL. Sildenafil ameliorates effects of inhaled nitric oxide withdrawal. Anesthesiology. 1999;91:307–10. - PubMed
-
- Aubert S, Leprince P, Bonnet N, et al. Limited mechanical circulatory support following orthotopic heart transplantation. Interact Cardiovasc Thorac Surg. 2006;5:88–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
