

Hemorrhage-induced hepatic injury and hypoperfusion can be prevented by direct peritoneal resuscitation
- PMID: 19184613
- PMCID: PMC2715546
- DOI: 10.1007/s11605-008-0796-0
Hemorrhage-induced hepatic injury and hypoperfusion can be prevented by direct peritoneal resuscitation
Abstract
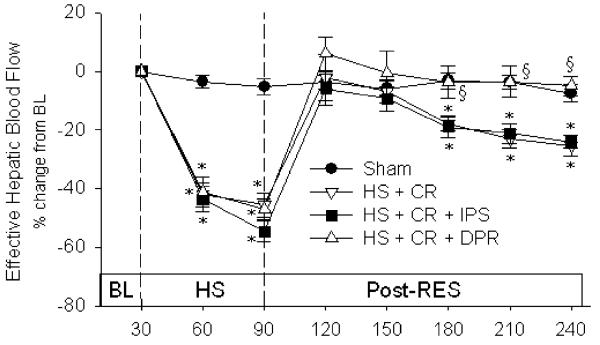
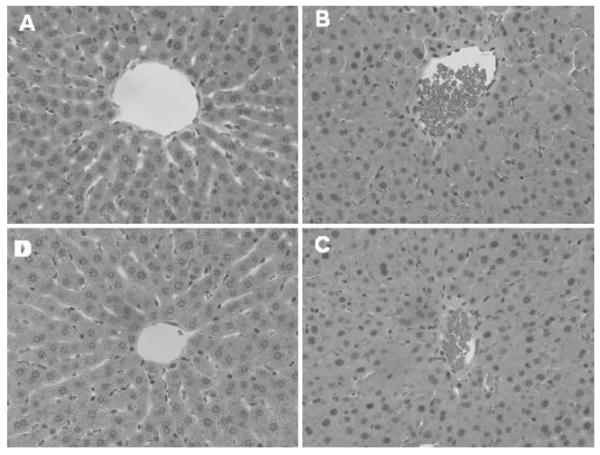
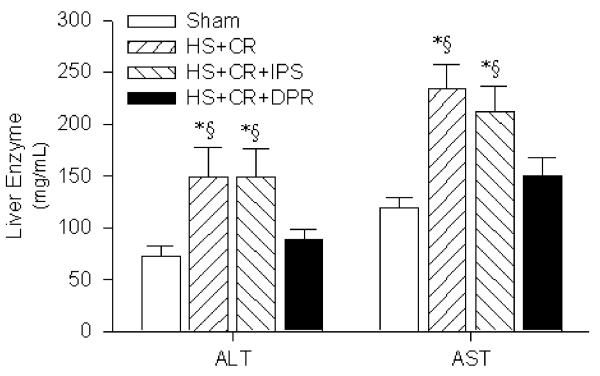
Background: Crystalloid fluid resuscitation after hemorrhagic shock (HS) that restores/maintains central hemodynamics often culminates in multi-system organ failure and death due to persistent/progressive splanchnic hypoperfusion and end-organ damage. Adjunctive direct peritoneal resuscitation (DPR) using peritoneal dialysis solution reverses HS-induced splanchnic hypoperfusion and improves survival. We examined HS-mediated hepatic perfusion (galactose clearance), tissue injury (histopathology), and dysfunction (liver enzymes).
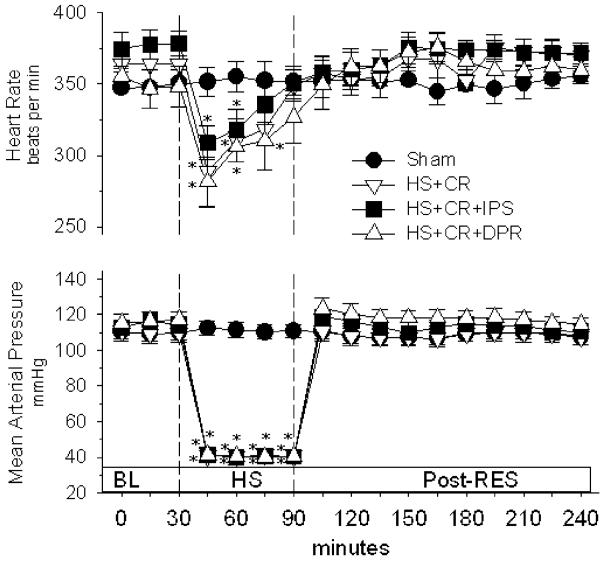
Methods: Anesthetized rats were randomly assigned (n = 8/group): (1) sham (no HS); (2) HS (40% mean arterial pressure for 60 min) plus conventional i.v. fluid resuscitation (CR; shed blood + 2 volumes saline); (3) HS + CR + 30 mL intraperitoneal (IP) DPR; or (4) HS + CR + 30 mL IP saline. Hemodynamics and hepatic blood flow were measured for 2 h after CR completion. In duplicate animals, liver and splanchnic tissues were harvested for histopathology (blinded, graded), hepatocellular function (liver enzymes), and tissue edema (wet-dry ratio).
Results: Group 2 decreased liver blood flow, caused liver injuries (focal to submassive necrosis, zones 2 and 3) and tissue edema, and elevated liver enzymes (alanine aminotransferase (ALT), 149 +/- 28 microg/mL and aspartate aminotransferase (AST), 234 +/- 24 microg/mL; p < 0.05) compared to group 1 (73 +/- 9 and 119 +/- 10 microg/mL, respectively). Minimal/no injuries were observed in group 3; enzymes were normalized (ALT 89 +/- 9 microg/mL and AST 150 +/- 17 microg/mL), and tissue edema was similar to sham.
Conclusions: CR from HS restored and maintained central hemodynamics but did not restore or maintain liver perfusion and was associated with significant hepatocellular injury and dysfunction. DPR added to conventional resuscitation (blood and crystalloid) restored and maintained liver perfusion, prevented hepatocellular injury and edema, and preserved liver function.
Figures

References
-
- Hassoun HT, Kone BC, Mercer DW, Moody FG, Weisbrodt NW, Moore FA. Post-injury multiple organ failure: the role of the gut. Shock. 2001;15:1–10. - PubMed
-
- Fruchterman TM, Spain DA, Wilson MA, Harris PD, Garrison RN. Selective microvascular endothelial cell dysfunction in the small intestine following resuscitated hemorrhagic shock. Shock. 1998;10:417–422. doi:10.1097/00024382-199812000-00007. - PubMed
-
- Wang P, Hauptman JG, Chaudry IH. Hemorrhage produces depression in microvascular blood flow which persists despite fluid resuscitation. Circ Shock. 1990;32:307–318. - PubMed
-
- Zakaria ER, Spain DA, Harris PD, Garrison RN. Resuscitation regimens for hemorrhagic shock must contain blood. Shock. 2002;18:567–573. doi:10.1097/00024382-200212000-00014. - PubMed
-
- Deitch EA, Xu D, Franko L, Ayala A, Chaudry IH. Evidence favoring the role of the gut as a cytokine-generating organ in rats subjected to hemorrhagic shock. Shock. 1994;1:141–145. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
