

Fetal renal artery impedance as assessed by Doppler ultrasound in pregnancies complicated by intraamniotic inflammation and preterm birth
- PMID: 19185102
- PMCID: PMC3791328
- DOI: 10.1016/j.ajog.2008.11.001
Fetal renal artery impedance as assessed by Doppler ultrasound in pregnancies complicated by intraamniotic inflammation and preterm birth
Abstract
Objective: The objective of the study was to evaluate the fetal renal artery impedance in the context of inflammation-associated preterm birth.
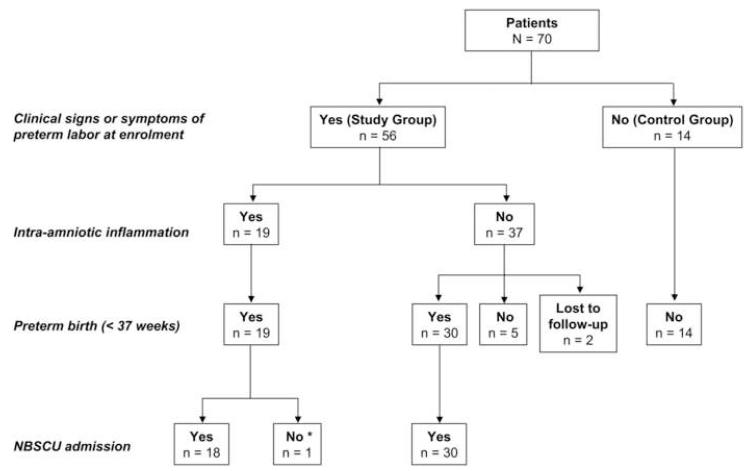
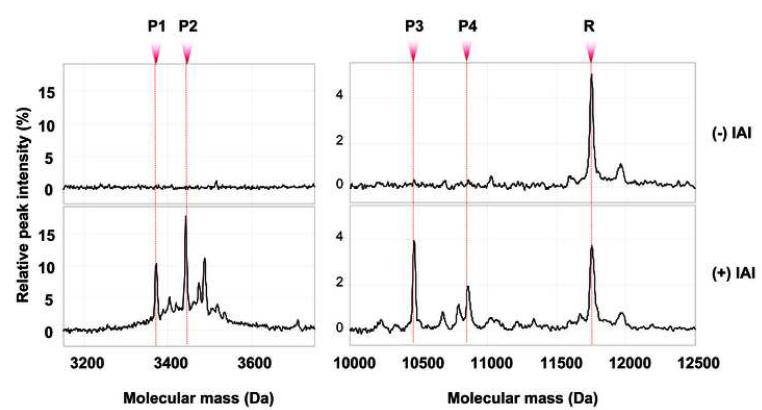
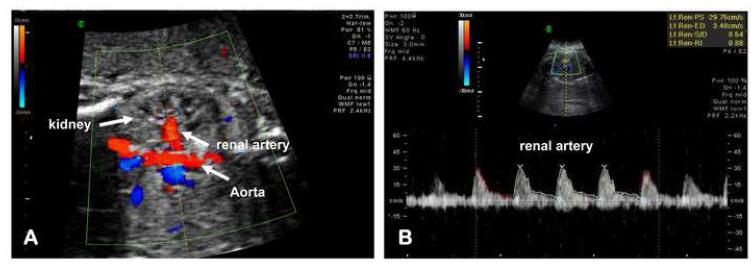
Study design: We conducted a prospective Doppler assessment of the fetal renal artery impedance in 70 singleton fetuses. The study group consisted of 56 premature fetuses (median, 28.1 [interquartile range, 25.3-30.6] weeks at enrollment). Gestational age (GA) reference ranges were generated based on fetuses with uncomplicated pregnancies (n = 14). Doppler studies included renal artery pulsatility index (PI), resistance index (RI), systolic/diastolic (S/D) ratio, and presence or absence of end-diastolic blood flow. Proteomic profiling (surface-enhanced laser desorption ionization time-of-flight) was used for assessment of intraamniotic inflammation and biomarker peak corresponding to beta2-microglubin. Data were interpreted in relationship to amniotic fluid index (AFI), cord blood interleukin (IL)-6 and erythropoietin (EPO) levels. The cardiovascular and metabolic profiles of the neonates were investigated in the first 24 hours of life.
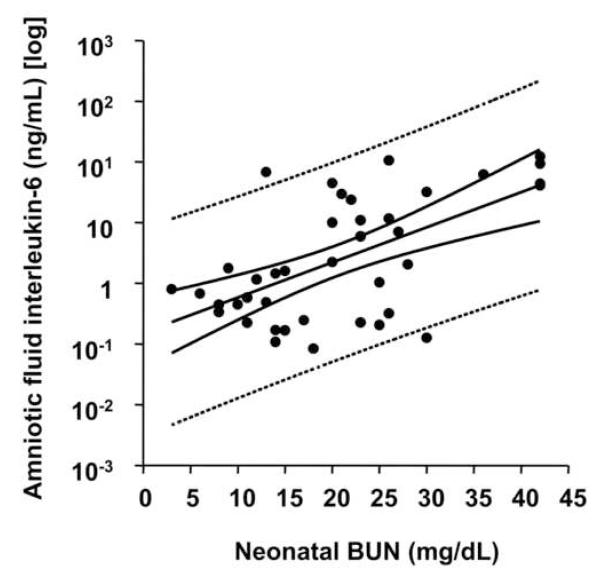
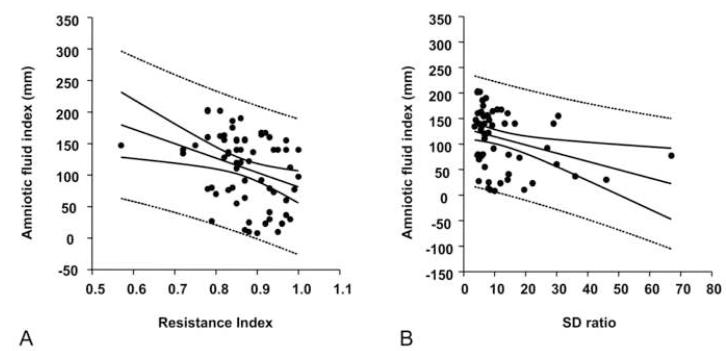
Results: Fetuses delivered by mothers with intraamniotic inflammation had higher cord blood IL-6 but not EPO levels. Fetal inflammation did not affect either renal artery PI, RI, S/D ratio, or end-diastolic blood flow. Neonates delivered in the context of intraamniotic inflammation had higher serum blood urea nitrogen levels, which correlated significantly with AF IL-6 levels. The renal artery RI and SD ratio were inversely correlated with the AFI independent of GA, cord blood IL-6, and status of the membranes.
Conclusion: The fetus is capable of sustaining normal renal artery impedance despite inflammation. Resistance in the renal vascular bed affects urine output independent of inflammation.
Figures
Similar articles
-
Fetal inflammatory response in women with proteomic biomarkers characteristic of intra-amniotic inflammation and preterm birth.BJOG. 2009 Jan;116(2):257-67. doi: 10.1111/j.1471-0528.2008.01925.x. Epub 2008 Oct 8. BJOG. 2009. PMID: 18947340 Free PMC article.
-
Intra-amniotic infection and/or inflammation is associated with fetal cardiac concentric hypertrophy and diastolic dysfunction in preterm labor and preterm prelabor rupture of membranes.Am J Obstet Gynecol. 2024 Jun;230(6):665.e1-665.e30. doi: 10.1016/j.ajog.2023.10.017. Epub 2024 Jan 9. Am J Obstet Gynecol. 2024. PMID: 38290925
-
Evidence of brain injury in fetuses of mothers with preterm labor with intact membranes and preterm premature rupture of membranes.Am J Obstet Gynecol. 2025 Jan;232(1):114.e1-114.e24. doi: 10.1016/j.ajog.2024.04.025. Epub 2024 Apr 27. Am J Obstet Gynecol. 2025. PMID: 38685550
-
Maternal azithromycin therapy for Ureaplasma parvum intraamniotic infection improves fetal hemodynamics in a nonhuman primate model.Am J Obstet Gynecol. 2020 Oct;223(4):578.e1-578.e11. doi: 10.1016/j.ajog.2020.04.015. Epub 2020 Apr 25. Am J Obstet Gynecol. 2020. PMID: 32343954 Free PMC article.
-
The prevalence and clinical significance of intraamniotic infection with Candida species in women with preterm labor.Arch Gynecol Obstet. 1992;251(1):9-15. doi: 10.1007/BF02718273. Arch Gynecol Obstet. 1992. PMID: 1550392 Review.
Cited by
-
Characterization of RAGE, HMGB1, and S100beta in inflammation-induced preterm birth and fetal tissue injury.Am J Pathol. 2009 Sep;175(3):958-75. doi: 10.2353/ajpath.2009.090156. Epub 2009 Aug 13. Am J Pathol. 2009. PMID: 19679874 Free PMC article.
-
The fetal inflammatory response syndrome: the origins of a concept, pathophysiology, diagnosis, and obstetrical implications.Semin Fetal Neonatal Med. 2020 Aug;25(4):101146. doi: 10.1016/j.siny.2020.101146. Epub 2020 Oct 23. Semin Fetal Neonatal Med. 2020. PMID: 33164775 Free PMC article.
-
Systemic Inflammatory Response Syndrome, Thromboinflammation, and Septic Shock in Fetuses and Neonates.Int J Mol Sci. 2025 Apr 1;26(7):3259. doi: 10.3390/ijms26073259. Int J Mol Sci. 2025. PMID: 40244141 Free PMC article. Review.
References
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371:261–9. - PubMed
-
- Lawn JE, Cousens S, Zupan J. Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: when? Where? Why? Lancet. 2005;365:891–900. - PubMed
-
- Lockwood CJ, Kuczynski E. Risk stratification and pathological mechanisms in preterm delivery. Paediatr Perinat Epidemiol. 2001;15:78–89. - PubMed
-
- Buhimschi CS, Rosenberg VA, Dulay AT, Thung S, Sfakianaki AK, Bahtiyar MO, Buhimschi IA. Multidimensional system biology. Genetic and proteomic biomarkers of adverse pregnancy outcome in preterm birth. Am J Perinatol. 2008;25:175–87. - PubMed
-
- Buhimschi IA, Zambrano E, Pettker CM, Bahtiyar MO, Paidas M, Rosenberg VA, et al. Using proteomic analysis of the human amniotic fluid to identify histological chorioamnionitis. Obstet Gynecol. 2008;111:403–412. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
