

Effects of on- and off-pump coronary artery surgery on graft patency, survival, and health-related quality of life: long-term follow-up of 2 randomized controlled trials
- PMID: 19185140
- PMCID: PMC2836483
- DOI: 10.1016/j.jtcvs.2008.09.046
Effects of on- and off-pump coronary artery surgery on graft patency, survival, and health-related quality of life: long-term follow-up of 2 randomized controlled trials
Abstract
Objective: Off-pump coronary artery bypass grafting reduces postoperative morbidity and uses fewer resources than conventional surgical intervention with cardiopulmonary bypass. However, only 15% to 20% of coronary artery bypass grafting operations use off-pump coronary artery bypass. One reason for not using off-pump coronary artery bypass might be the surgeon's concern about the long-term patency of grafts performed with this technique. Therefore our objective was to compare long-term outcomes in patients randomized to off-pump coronary artery bypass or coronary artery bypass grafting with cardiopulmonary bypass.
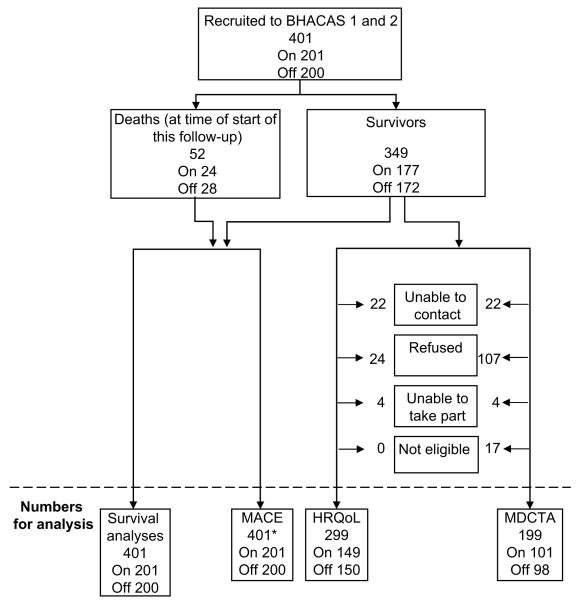
Methods: Participants in 2 randomized trials comparing off-pump coronary artery bypass and coronary artery bypass grafting with cardiopulmonary bypass were followed up for 6 to 8 years after surgical intervention to assess graft patency, major adverse cardiac-related events, and health-related quality of life. Patency was assessed by using multidetector computed tomographic coronary angiographic analysis with a 16-slice scanner. Two blinded observers classified proximal, body, and distal segments of each graft as occluded or not. Major adverse cardiac-related events and health-related quality of life were obtained from questionnaires given to participants and family practitioners.
Results: Patency was studied in 199 and health-related quality of life was studied in 299 of 349 survivors. There was no evidence of attrition bias. The likelihood of graft occlusion was no different between off-pump coronary artery bypass (10.6%) and coronary artery bypass grafting with cardiopulmonary bypass (11.0%) groups (odds ratio, 1.00; 95% confidence interval, 0.55-1.81; P > .99). Graft occlusion was more likely at the distal than the proximal anastomosis (odds ratio, 1.11; 95% confidence interval, 1.02-1.20). There were also no differences between the off-pump coronary artery bypass and coronary artery bypass grafting with cardiopulmonary bypass groups in the hazard of death (hazard ratio, 1.24; 95% confidence interval, 0.72-2.15) or major adverse cardiac-related events or death (hazard ratio, 0.84; 95% confidence interval, 0.58-1.24), or mean health-related quality of life across a range of domains and instruments.
Conclusions: Long-term health outcomes with off-pump coronary artery bypass are similar to those with coronary artery bypass grafting with cardiopulmonary bypass when both operations are performed by experienced surgeons.
Figures

Comment in
-
Graft patency in coronary artery bypass versus off-pump coronary artery bypass.J Thorac Cardiovasc Surg. 2009 Sep;138(3):792-3; author reply 793-4. doi: 10.1016/j.jtcvs.2009.04.051. J Thorac Cardiovasc Surg. 2009. PMID: 19698889 No abstract available.
References
-
- Cheng DC, Bainbridge D, Martin JE, Novick RJ. Evidence based perioperative clinical outcomes research group. Does off-pump coronary artery bypass reduce mortality, morbidity, and resource utilization when compared with conventional coronary artery bypass? A meta-analysis of randomized trials. Anesthesiology. 2005;102:188–203. - PubMed
-
- Wijeysundera DN, Beattie WS, Djaiani G, Rao V, Borger MA, Karkouti K, et al. Off pump coronary artery surgery for reducing mortality and morbidity: meta-analysis of randomized and observational studies. J Am Coll Cardiol. 2005;46:872–82. - PubMed
-
- Ascione R, Lloyd CT, Underwood MJ, Lotto AA, Pitsis AA, Angelini GD. Economic outcome of off-pump coronary artery bypass surgery: a prospective randomized study. Ann Thorac Surg. 1999;68:2237–42. - PubMed
-
- Puskas JD, Williams WH, Mahoney EM, Huber PR, Block PC, Duke PG, et al. Off-pump vs. conventional coronary artery bypass grafting: early and 1-year graft patency, cost, and quality-of-life outcomes: a randomized trial. JAMA. 2004;291:1841–9. - PubMed
-
- Nathoe HM, van Dijk D, Jansen EWL, Suyker WJ, Diephuis JC, van Boven WJ, et al. A comparison of on-pump and off-pump coronary bypass surgery in lowrisk patients. N Engl J Med. 2003;348:394–402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
