

A multifaceted intervention to improve blood pressure control: The Guideline Adherence for Heart Health (GLAD) study
- PMID: 19185634
- PMCID: PMC2929708
- DOI: 10.1016/j.ahj.2008.09.021
A multifaceted intervention to improve blood pressure control: The Guideline Adherence for Heart Health (GLAD) study
Abstract
Background: Although high blood pressure is associated with significant morbidity and mortality, the proportion reaching the goal blood pressures as outlined in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, Treatment of High Blood Pressure (JNC 7) is low. We conducted a randomized trial in primary care practices of a multifactorial intervention targeted to improve providers' adherence to hypertension guidelines.
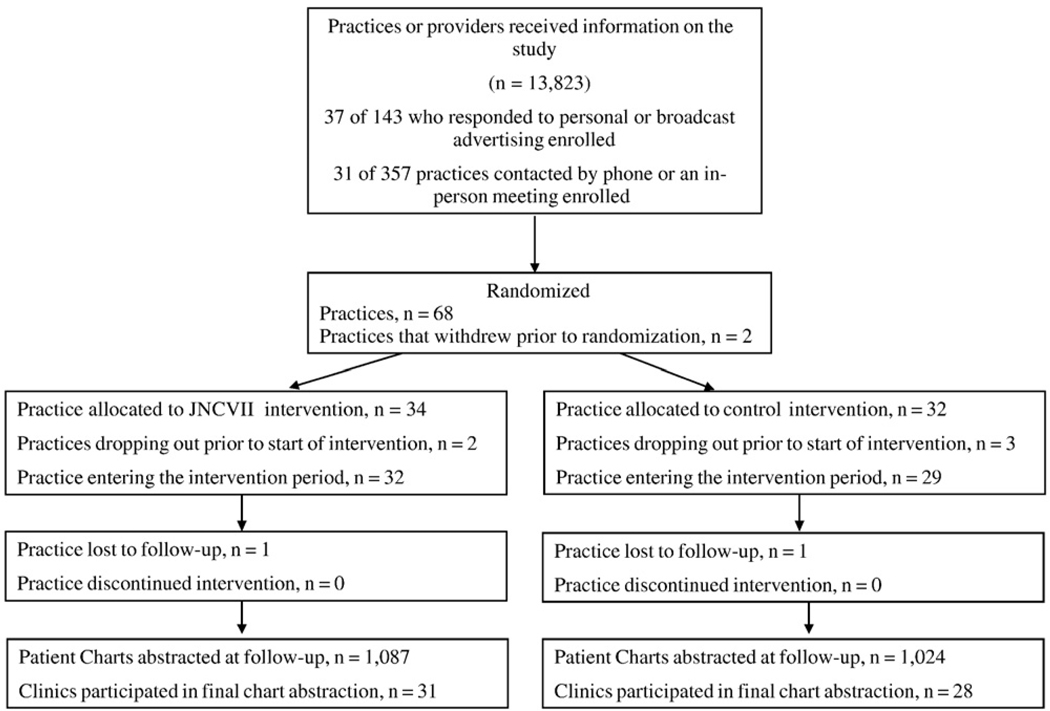
Method: A total of 61 primary care practices in North Carolina were randomized to receive either a multifactorial intervention (guideline dissemination via a continuing medical education session, academic detailing sessions, audit and feedback on preintervention rates of adherence, and automated blood pressure machines) or an attention control of similar magnitude but targeted at a different guideline. Outcomes were determined through review of patient charts conducted by an independent masked quality assurance organization.
Results: We found no difference between the 2 groups in any of the adherence measures including no difference in the percentage of patients at goal (intervention 49.2%, control 50.6%), with undiagnosed hypertension (18.1% vs 13.6%), average systolic (126 vs 125.1 mm Hg), or diastolic blood pressure (73.1 vs 73.4 mm Hg). Similarly, there was no difference in provider adherence to treatment recommendations (use of thiazide-type diuretic as first-line therapy: 32% vs 29.5%; use of 2-drug therapy in stage 2 hypertension: 11.3% vs 10.4%).
Conclusion: An intensive, multifactorial intervention did not improve adherence to national hypertension guidelines among community-based primary care. Efforts should be focused on other types of interventions to improve rates of control of hypertension.
Figures
References
-
- Ong KL, Cheung BM, Man YB, et al. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999–2004. Hypertension. 2007;49:69–75. - PubMed
-
- Thom T, Haase N, Rosamond W, et al. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113:e85–e151. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–1252. - PubMed
-
- Thier SL, Yu-Isenberg KS, Leas BF, et al. In chronic disease, nationwide data show poor adherence by patients to medication and by physicians to guidelines. Manag Care. 2008;17:48–52. 55–57. - PubMed
-
- Cabana MD, Rand CS, Powe NR, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282:1458–1465. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
