

Review
doi: 10.1016/j.tcm.2008.11.002.
Congenital long-QT syndromes: a clinical and genetic update from infancy through adulthood
Affiliations
- PMID: 19185812
- PMCID: PMC4260467
- DOI: 10.1016/j.tcm.2008.11.002
Item in Clipboard
Review
Congenital long-QT syndromes: a clinical and genetic update from infancy through adulthood
Trends Cardiovasc Med.
2008 Aug.
Abstract
Long-QT syndromes (LQTSs) have been described in all ages and are a significant cause of cardiovascular mortality, especially in structurally normal hearts. Abnormalities in transmembrane ion conduction channels and structural proteins produce these clinical syndromes, labeled LQT1-LQT12; however, genotype-positive patients still represent only about 70% of LQTSs. Future research will determine the etiology of the remaining cases, further risk-stratify the known genetic defects, improve current treatment options for these syndromes, and uncover novel therapies.
Figures
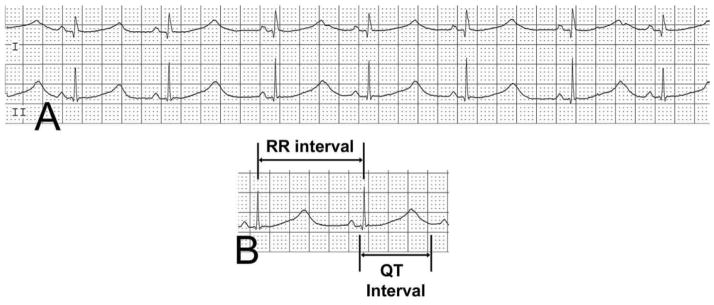
Surface ECG showing a prolonged QTc of 687. Measurement of the QTc is calculated as the duration of the QT interval, divided by the square root of the preceding RR interval.

Surface ECG rhythm strip showing a QTc of 675 and 2:1 atrioventricular block.
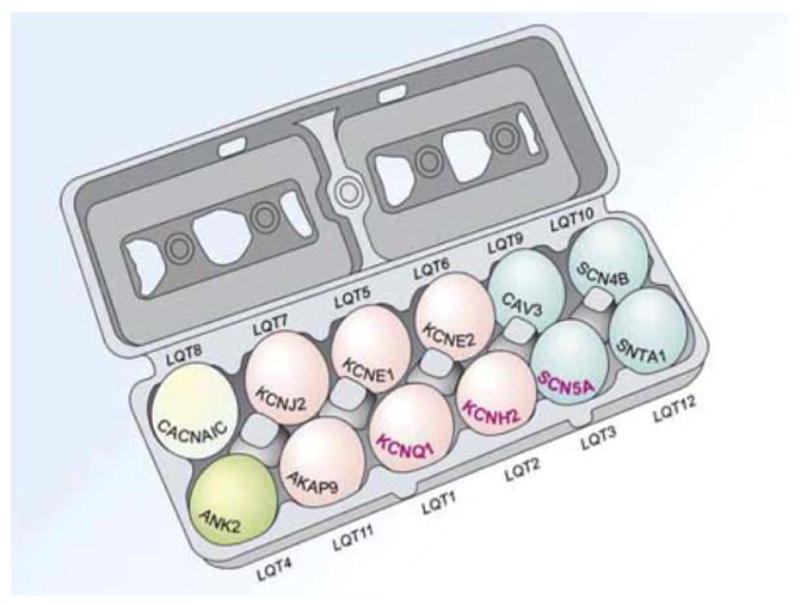
Cartoon diagram of the 12 known LQTS genes and the LQT syndromes associated with mutations in each gene (LQT1-LQT12). The 3 most common (LQT1-3) are in bold. Eggs are color-coded by the functionality of each gene and its respective protein: pink, potassium channel; blue, sodium channel; green, calcium channel; ivory, structural protein.
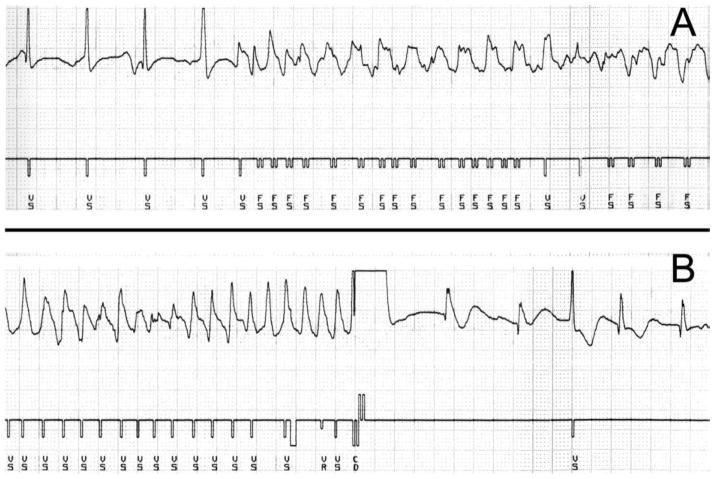
(A) ICD ventricular intracardiac electrogram and a marker channel. The electrogram begins with sinus rhythm at a ventricular rate of 100 beats per minute with sudden initiation of a polymorphic ventricular rhythm at a rate of approximately 215 beats per minute. The marker channel assigns the electrical deflections as ventricular sensing (VS) and ventricular fibrillation detection (FS). (B) Ventricular intracardiac electrogram recording demonstrating successful ICD shock. The electrogram shows polymorphic ventricular tachycardia with a rate of 300 beats per minute. The marker channel assigns the electrical deflections as ventricular sensing (VS) and refractory (VR). The device discharges (CD) and the rhythm returns to a ventricular rate of approximately 110 beats per minute.
References
-
- Al-Khatib SM, LaPointe NM, Kramer JM, Califf RM. What clinicians should know about the QT interval. JAMA. 2003;289:2120–2127. - PubMed
-
- Atallah J, Fynn-Thompson F, Cecchin F, et al. Video-assisted thoracoscopic cardiac denervation: a potential novel therapeutic option for children with intractable ventricular arrhythmias. Ann Thorac Surg. 2008;86:1620–1625. - PubMed
-
- Berul CI, Sweeten TL, Dubin, et al. Use of the rate-corrected JT interval for prediction of repolarization abnormalities in children. Am J Cardiol. 1994;74:1254–1257. - PubMed
-
- Berul CI, Sweeten TL, Hill SL, Vetter VL. Provocative testing in children with suspect congenital long QT syndrome. Ann Noninvasive Electrocardiol. 1998;3:3–11.
-
- Crotti L, Spazzolini C, Schwartz PJ, et al. The common long-QT syndrome mutation KCNQ1/A341V causes unusually severe clinical manifestations in patients with different ethnic backgrounds: toward a mutation-specific risk stratification. Circulation. 2007;116:2366–2375. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
