

Acute exacerbations of asthma: epidemiology, biology and the exacerbation-prone phenotype
- PMID: 19187331
- PMCID: PMC2730743
- DOI: 10.1111/j.1365-2222.2008.03157.x
Acute exacerbations of asthma: epidemiology, biology and the exacerbation-prone phenotype
Abstract
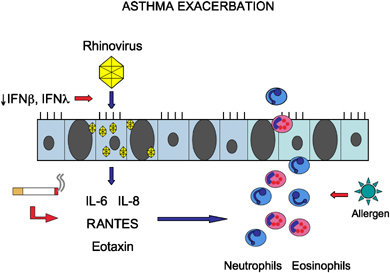
Asthma is a highly prevalent chronic respiratory disease affecting 300 million people world-wide. A significant fraction of the cost and morbidity of asthma derives from acute care for asthma exacerbations. In the United States alone, there are approximately 15 million outpatient visits, 2 million emergency room visits, and 500,000 hospitalizations each year for management of acute asthma. Common respiratory viruses, especially rhinoviruses, cause the majority of exacerbations in children and adults. Infection of airway epithelial cells with rhinovirus causes the release of pro-inflammatory cytokines and chemokines, as well as recruitment of inflammatory cells, particularly neutrophils, lymphocytes, and eosinophils. The host response to viral infection is likely to influence susceptibility to asthma exacerbation. Having had at least one exacerbation is an important risk factor for recurrent exacerbations suggesting an 'exacerbation-prone' subset of asthmatics. Factors underlying the 'exacerbation-prone' phenotype are incompletely understood but include extrinsic factors: cigarette smoking, medication non-compliance, psychosocial factors, and co-morbidities such as gastroesophageal reflux disease, rhinosinusitis, obesity, and intolerance to non-steroidal anti-inflammatory medications; as well as intrinsic factors such as deficient epithelial cell production of the anti-viral type I interferons (IFN-alpha and IFN-beta). A better understanding of the biologic mechanisms of host susceptibility to recurrent exacerbations will be important for developing more effective preventions and treatments aimed at reducing the significant cost and morbidity associated with this important global health problem.
Figures

References
-
- O'Byrne PM, Barnes PJ, Rodriguez‐Roisin R et al Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med 2001; 164 (Part 1):1392–7. - PubMed
-
- Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 2004; 59:469–78. - PubMed
-
- CDC National Center for Health Statistics. Asthma prevalence, health care use and mortality: United States, 2003–05 [cited]; available from: http://www.cdc.gov/nchs/products/pubs/pubd/hestats/ashtma03-05/asthma03-...
-
- Rodrigo GJ, Rodrigo C, Hall JB. Acute asthma in adults: a review. Chest 2004; 125:1081–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
