

Risk of postpartum depressive symptoms with elevated corticotropin-releasing hormone in human pregnancy
- PMID: 19188538
- PMCID: PMC2768579
- DOI: 10.1001/archgenpsychiatry.2008.533
Risk of postpartum depressive symptoms with elevated corticotropin-releasing hormone in human pregnancy
Abstract
Context: Postpartum depression (PPD) is common and has serious implications for the mother and her newborn infant. A possible link between placental corticotropin-releasing hormone (pCRH) and PPD incidence has been hypothesized, but empirical evidence is lacking.
Objective: To determine whether accelerated increases in pCRH throughout pregnancy are associated with PPD symptoms.
Design: Pregnant women were recruited into this longitudinal cohort study. Blood samples were obtained at 15, 19, 25, 31, and 37 weeks' gestational age (GA) for assessment of pCRH, cortisol, and adrenocorticotropic hormone (ACTH). Depressive symptoms were assessed with a standardized questionnaire at the last 4 pregnancy visits and post partum.
Setting: Subjects were recruited from 2 southern California medical centers, and visits were conducted in research laboratories.
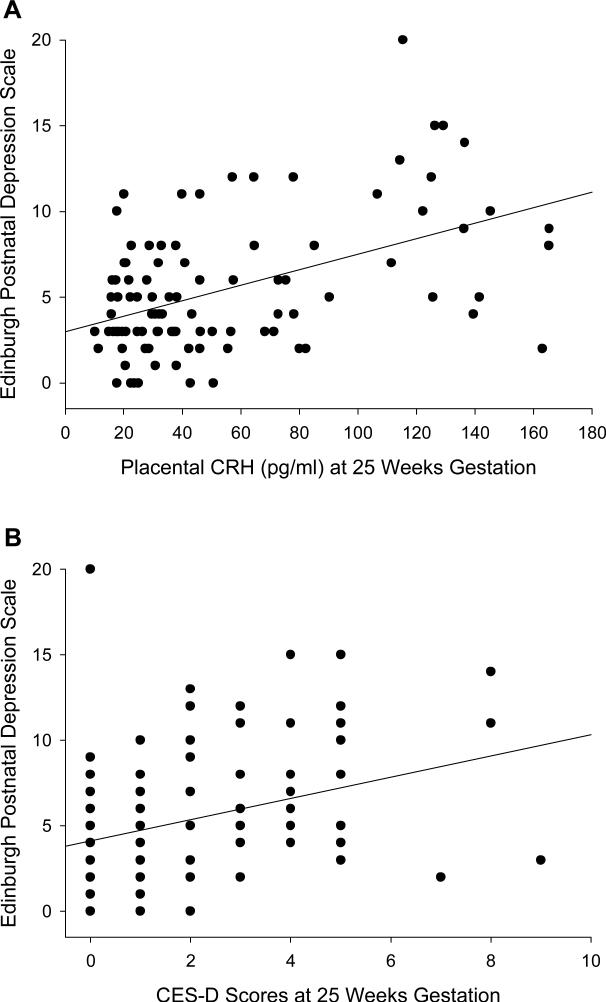
Participants: One hundred adult women with a singleton pregnancy. Main Outcome Measure Symptoms of PPD were assessed at a mean (SD) of 8.7 (2.94) weeks after delivery with the Edinburgh Postnatal Depression Scale.
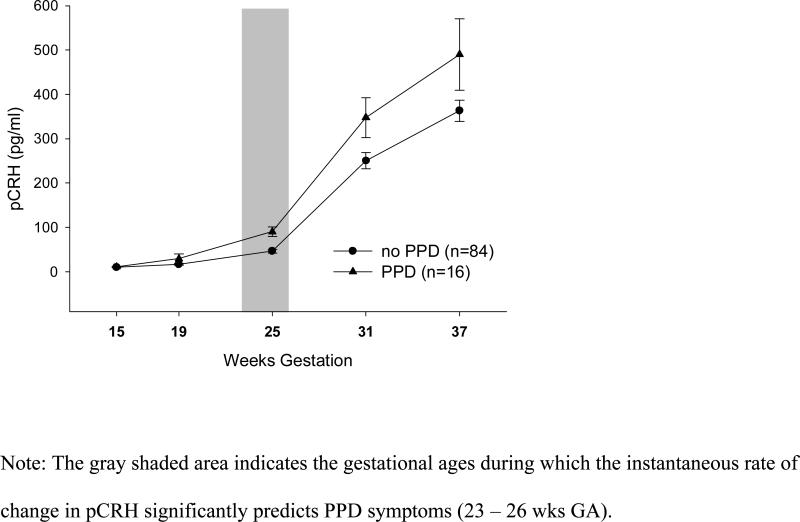
Results: Sixteen women developed PPD symptoms. At 25 weeks' GA, pCRH was a strong predictor of PPD symptoms (R(2) = 0.21; beta = 0.46 [P < .001]), an effect that remained significant after controlling for prenatal depressive symptoms. No significant associations were found for cortisol and ACTH. Receiver operating characteristic curve analyses revealed that pCRH at 25 weeks' GA is a possible diagnostic tool (area under the curve, 0.78 [P = .001]). Sensitivity (0.75) and specificity (0.74) at the ideal cutoff point (pCRH, 56.86 pg/mL) were moderate. Growth curve analyses indicated that the trajectories of pCRH in women with PPD symptoms are significantly accelerated from 23 to 26 weeks' GA.
Conclusions: At a critical period in midpregnancy, pCRH is a sensitive and specific early diagnostic test for PPD symptoms. If replicated, these results have implications for the identification and treatment of pregnant women at risk for PPD.
Figures


Comment in
-
Premature recommendation of corticotropin-releasing hormone as screen for postpartum depression.Arch Gen Psychiatry. 2009 Aug;66(8):917. doi: 10.1001/archgenpsychiatry.2009.101. Arch Gen Psychiatry. 2009. PMID: 19652134 Free PMC article. No abstract available.
References
-
- Brockington I. Postpartum psychiatric disorders. Lancet. 2004;363(9405):303–310. - PubMed
-
- World Health Organization . The international statistical classification of diseases and related health problems. 10 ed. World Health Organization; Geneva, Switzerland: 1992.
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4 ed. American Psychiatric Press; Washington (DC): 1994.
-
- Grace SL, Evindar A, Stewart DE. The effect of postpartum depression on child cognitive development and behavior: a review and critical analysis of the literature. Arch Womens Ment Health. 2003;6(4):263–274. - PubMed
-
- Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol. 2005;106(5 Pt 1):1071–1083. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
