

Technical performance and reflection capacity of the anaesthetic conserving device--a bench study with isoflurane and sevoflurane
- PMID: 19189222
- PMCID: PMC2799001
- DOI: 10.1007/s10877-008-9158-4
Technical performance and reflection capacity of the anaesthetic conserving device--a bench study with isoflurane and sevoflurane
Abstract
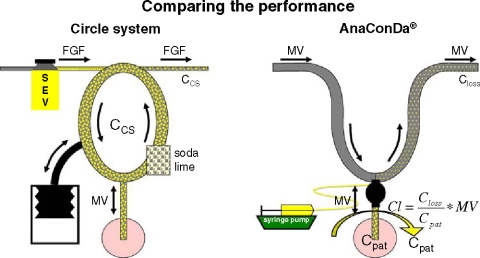
Objective: The anaesthetic conserving device (AnaConDa), Sedana Medical, Sundbyberg, Sweden) facilitates administration of isoflurane or sevoflurane by liquid infusion. An anaesthetic reflector inside the device conserves exhaled anaesthetic and re-supplies it during inspiration. In this bench study, we examined the influence of infusion rates and ventilatory settings on the resulting anaesthetic concentrations on patient (C(pat)) and ventilator side of the reflector (C(loss)) to describe its technical performance.
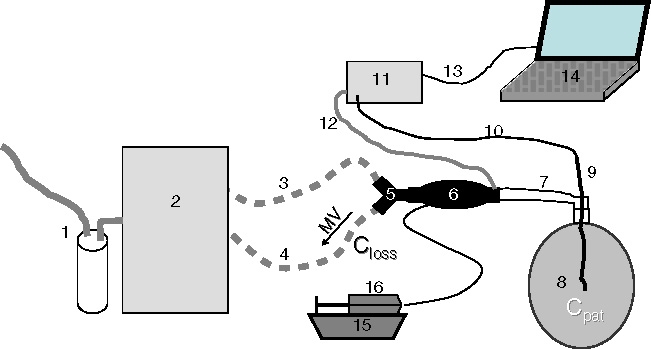
Methods: A Puritan Bennett 840 ICU ventilator (Pleasanton, US), AnaConDa, and a test lung (3 l-chloroprene-bag) were assembled. Infusion rates (IR, 0.2-50 ml h(-1)), respiratory rates (RR, 5-40 breaths min(-1)), and tidal volumes (V(T), 0.3, 0.5, and 1.0 l) were varied. C(pat) was measured via a thin catheter in the middle of the 3 l-bag in steady state (online data storage and averaging over >10 min). C(loss) was calculated from IR (to yield the volume of vapour per unit of time), and expired minute volume (in which the vapour is diluted) on the assumption that, in the steady state, input by liquid infusion equals output through the reflector.
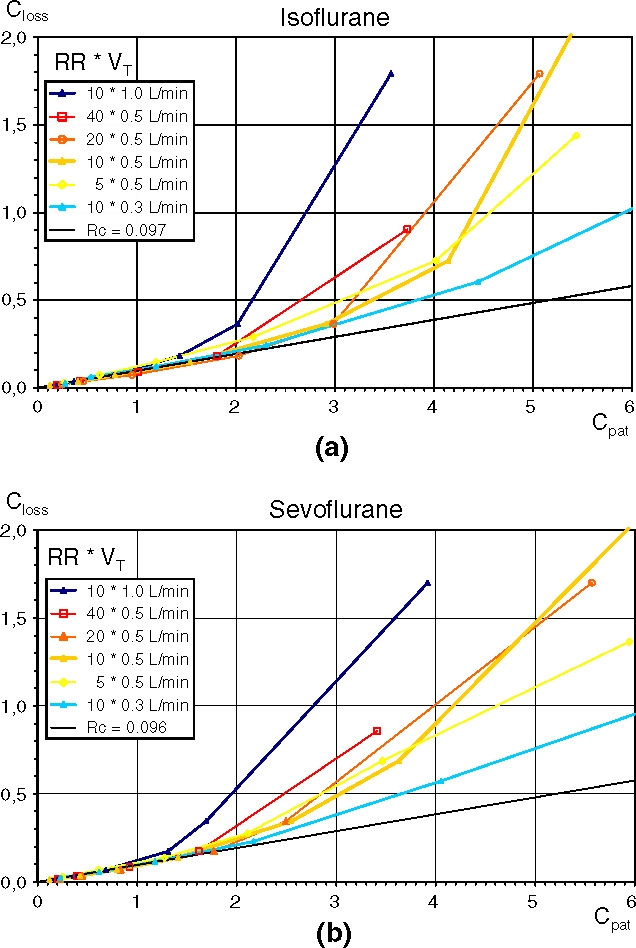
Results: At lower concentrations (C(pat) < 1 vol%) the ratio C(loss)/C(pat) was constant (R(C) = 0.096 +/- 0.012) for all combinations of IR, RR and V(T), both for isoflurane and sevoflurane. The device could efficiently reflect up to 10 ml vapour per breath (e.g. 2 vol% in 0.5 l). When exceeding this capacity, surplus vapour "spilled over" and R(C) markedly increased indicating decreased performance.
Conclusions: The triple product minute volume times R(C) times C(pat) describes anaesthetic losses through the reflector. It can easily be calculated as long as the 10 ml reflection capacity is not exceeded and thus R(C) is constant. Increased minute ventilation necessitates increasing the IR to keep C(pat) constant. When using large V(T) and high C(pat) "spill over" occurs. This effect offers some protection against an inadvertent overdose.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1046/j.1365-2044.2001.01900.x', 'is_inner': False, 'url': 'https://doi.org/10.1046/j.1365-2044.2001.01900.x'}, {'type': 'PubMed', 'value': '11350327', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11350327/'}]}
- Enlund M, Wiklund L, Lambert H. A new device to reduce the consumption of a halogenated anaesthetic agent. Anaesthesia 2001; 56: 429–432. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '15640636', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15640636/'}]}
- Sackey PV, Martling CR, Granath F, Radell PJ. Prolonged isoflurane sedation of intensive care unit patients with the Anesthetic Conserving Device. Crit Care Med 2004; 32: 2241–2246. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1111/j.1365-2044.2007.05010.x', 'is_inner': False, 'url': 'https://doi.org/10.1111/j.1365-2044.2007.05010.x'}, {'type': 'PubMed', 'value': '17300319', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17300319/'}]}
- Thomson H, Harper NJ, Parkes A. Use of the AnaConDa anaesthetic delivery system to treat life-threatening asthma. Anaesthesia 2007; 62: 295–296. - PubMed
-
- Jung C, Granados M, Marsol P, Murat I, Gall O. Use of sevoflurane sedation by the AnaConDa((R)) device as an adjunct to extubation in a pediatric burn patient. Burns 2008; 34: 136–138. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1007/s00101-007-1152-6', 'is_inner': False, 'url': 'https://doi.org/10.1007/s00101-007-1152-6'}, {'type': 'PubMed', 'value': '17375268', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17375268/'}]}
- Nickel EA, Benken I, Bartels U, Voelckel WG, Quintel M. AnaCoDa as last resort treatment. Case report of a chronic obstructive pulmonary disease. Anaesthesist 2007; 56: 587–591. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
